


U.S. Advanced Practice Registered Nurses (APRNs) are nationally certified but regulated by state law. States differ regarding scope of practice (SOP) restrictions imposed on APRNs. Little is known about provider attitudes toward these SOP-limiting policies in Ohio. This study was conducted in two phases. The first phase aimed to explore Ohio APRNs’ reported frustrations at work. The second phase further examined the most frequently reported frustration. A total of 262 Ohio APRNs participated in the survey. We expected that coronavirus concerns would be the most common work frustration, but that was not the case. The most frequently reported frustration was the law limiting APRN SOP in Ohio. This law was analyzed using the Theory of Planned Behavior to identify any links with actual behavior, including the frequency of collaborative events with the assigned physician (Ajzen, 1985, 1991). Frustration with state-mandated collaboration was found to be inversely related to the number of collaborative events. This leads to further investigation into APRN attitudes about mandatory collaboration in Ohio. Since most respondents are frustrated with the law, and collaboration decreases as frustration increases, more research is justified.
Key Words: barriers to practice, advanced practice nursing, scope of practice, policy, frustration, Ohio
Advanced practice registered nurses (APRNs) play a vital role in addressing healthcare access, quality, and workforce shortages in the United States. Although APRNs are nationally certified and highly educated to deliver quality care, their scope of practice is regulated at the state level, leading to significant variability in practice authority across the country. In states with restrictive or limited practice environments, laws requiring physician supervision or collaboration can influence how APRNs practice and view their professional roles. Ohio is one such state that mandates a standard care arrangement (SCA) between APRNs and physicians as a condition of practice. Despite long-standing policy debates about scope of practice regulations, little research has explored how these policies impact APRN attitudes, professional experiences, and collaborative behaviors. This study aims to examine Ohio APRNs’ reported workplace frustrations and analyze the relationship between frustration with mandated collaboration and the frequency of collaborative interactions with physicians, using the Theory of Planned Behavior as a conceptual framework.
Background
The year 2020 highlighted the working conditions of healthcare workers. The public, often only vaguely aware of the vital roles these professionals play, learned new terms that year, from “ventilator” to “personal protective equipment.” As nurses walked to work amid cheers and applause, the importance of nurses in our healthcare system, particularly advanced practice registered nurses (APRNs), was brought to light in new ways. In response to these challenges, as the pandemic subsided, the authors surveyed APRNs in Ohio to gather their opinions on their working conditions. The 21,842 APRNs, provided by the Ohio Board of Nursing, were surveyed and asked to comment on five potential sources of professional frustration (phase one of this study).
The five areas of possible professional frustration stem from the combined decades of APRN experience in Ohio by the first two authors. Frustration factors included: compensation, work hours, workload, coronavirus concerns, and the Ohio law requiring a collaborative agreement between APRNs and physicians, known as the standard care agreement (SCA). The responses revealed a surprising outcome. While it was expected that the coronavirus pandemic would be the primary source of frustration for these workers, the data instead showed that the Ohio SCA law, which mandates collaborative contracts between APRNs and similarly trained physicians, appears to contribute even more to their career frustrations. This variable became the focus of phase two of this study: analyzing the data statistically and considering the implications. This paper examines the data from this two-phase 2022 study and its insights into the law and its effects on APRN professional activities. The Theory of Planned Behavior (Ajzen, 1985, 1991) is used as a framework for analyzing these findings. The goal is that this initial report, along with future research, will enable the authors to suggest policy changes that help APRNs contribute optimally to public health.
What is an APRN?
Advanced practice registered nurses, or APRNs, are registered nurses with additional training through graduate degrees in a specialty area of nursing (American Nurses Association [ANA], 2017, Oct 19). The four recognized APRN types in the United States (U.S.) include nurse practitioners, clinical nurse specialists, nurse midwives, and certified registered nurse anesthetists (ANA, 2017, Oct 19). Nurse practitioners (NPs) are the largest practicing APRN type nationwide (ANA, 2017, Mar 9) and currently make up 42.9% of the U.S. primary care provider workforce (Davis, 2022).
Although APRNs are certified at the national level, licensure is handled by each state (ANA, 2017, Oct 20). States vary in their legal requirements for obtaining and maintaining licensure. Additionally, some states enact laws that restrict the roles APRNs can legally perform, known as the APRNs' scope of practice (SOP). There are notable differences among states concerning laws that limit APRNs' SOP (Zhang & Patel, 2022). The main method used to restrict APRNs' SOP involves mandatory contracts that specify a physician's supervision of an APRN's practice or require collaboration with a physician (Gilman et al., 2014; Martin & Alexander, 2019; Ruth et al., 2022). Deciding whether and how much to limit APRN SOP is a debate each state must resolve.
APRN SOP Debate
Deciding whether and how much to limit APRN SOP is a debate each state must resolve. The American Association of Nurse Practitioners (AANP, 2022, Map Legend) classifies three levels of practice environments based on restrictions on NPs' SOP, the APRN type with the largest national membership. "Full practice" states are those that allow NPs to practice fully, without laws limiting SOP, based on their education and training. "Restricted practice" states are the opposite, with laws explicitly reducing NPs' SOP by requiring physician supervision (AANP, 2022). "Reduced practice" states fall in between, where NPs need "regulated collaboration" with a physician to practice (AANP, 2022).
Numerous federal agencies, such as the National Academy of Sciences, Engineering, and Medicine (formerly the Institute of Medicine) and the Federal Trade Commission, have expressed support for “full practice authority” practice environments (National Academy of Sciences, Engineering, and Medicine, 2021, p. 87; Gilman et al., 2014). As the NP role has developed since its inception in 1965, the overall U.S. trend has been toward increased practice authority (Zhang & Patel, 2022). However, there is still significant variation from state to state. The AANP (2022, Map Legend) labels twenty-six U.S. states as "reduced practice” or “restricted practice” based on laws that limit NP SOP. The remaining states are classified as “full practice” states (AANP, 2022, Map Legend).
Groups opposing expanded APRN SOP often cite patient safety concerns. However, evidence supporting these concerns is lacking (Gilman et al., 2014). In contrast, extensive research shows that primary care outcomes for physicians and NPs are comparable. These findings have held true since the Senate Committee on Appropriations asked the U.S. Office of Technology Assessment in 1986 to study quality-of-care outcomes for NPs, nurse midwives, and physician assistants (Geller & Swan, 2021). Since then, outcome measures studied include: hospital admission rates, readmission rates, emergency department visits, heart failure measures, cholesterol levels, costs (Barnett et al., 2021), patient mortality rates (Barnett et al., 2021; Laurant et al., 2018), diabetes outcomes (Barnett et al., 2021; Everett et al., 2019; Jackson et al., 2018; Yang et al., 2017), blood pressure outcomes (Barnett et al., 2021; Htay & Whitehead, 2021; Laurant et al., 2018), indigestion, patients’ perception of health status, physical function (Htay & Whitehead, 2021), patient satisfaction (Barnett et al., 2021; Htay & Whitehead, 2021; Laurant et al., 2018), quality of life (Laurant et al., 2018), and prescribing practices (Jiao et al., 2018). ...extensive research shows that primary care outcomes for physicians and NPs are comparable.
Little has been reported regarding individual provider attitudes toward fuller NP SOP. One study from a Missouri sample of primary care providers (physicians and NPs) detailed support from each provider type for increased independence within primary care NP practice (Kraus & DuBois, 2017). Another review of the beliefs of NPs in Massachusetts one year after full practice authority was enacted found that NP respondents who reported improvements in patient care since full practice authority were significantly more likely (than those who did not report improvements) to find that timeliness, effectiveness, efficiency, and equity of care had benefited (O’Reilly-Jacob, et al., 2023). Even less evidence exists regarding APRN frustration levels as a result of state SOP limits. Ohio, which has “some of the strictest SOP laws in the country” (Martsolf et al., 2015, p. 2) and an APRN workforce numbering in the tens of thousands (Ohio Board of Nursing, no date), is a key candidate for further study of these phenomena.
Ohio and the SCA
Ohio is classified among the “reduced” practice states according to the AANP’s designations (2022, Map Legend). As a result, Ohio requires NPs to have “a career-long regulated collaborative agreement” with a physician to practice (AANP, 2022, Practice Environment Details under Map Legend). In Ohio, all APRNs—including NPs, clinical nurse specialists, and nurse midwives—must legally enter a standard care arrangement (SCA) with a “collaborating physician or podiatrist” of similar scope (Rule 4723-8-04, 2022, point H). Certified registered nurse anesthetists in Ohio are exempt from this requirement because their practice is supervised “under the direction of a podiatrist, a dentist, or a physician” (Rule 4723-8-01, 2021, point I). According to the Ohio Administrative Code, an SCA is a legal contract that details the names and contact information of the involved parties, the work location, an outline of the APRN's services, and quality assurance provisions related to those services (Rule 4723-8-04, 2022). The collaborating physician or podiatrist must be licensed in Ohio and hold a specialty similar to that of the APRN. The code does not specify the manner, frequency, or nature of the collaborative acts themselves. Additionally, there is limited guidance on how collaborators are selected. While Ohio APRNs who own their practices must seek out their collaborators, most employers choose the collaborator for APRN employees (Ohio Association of Advanced Practice Nurses [OAAPN], 2023).
Theoretical Underpinning of the Data
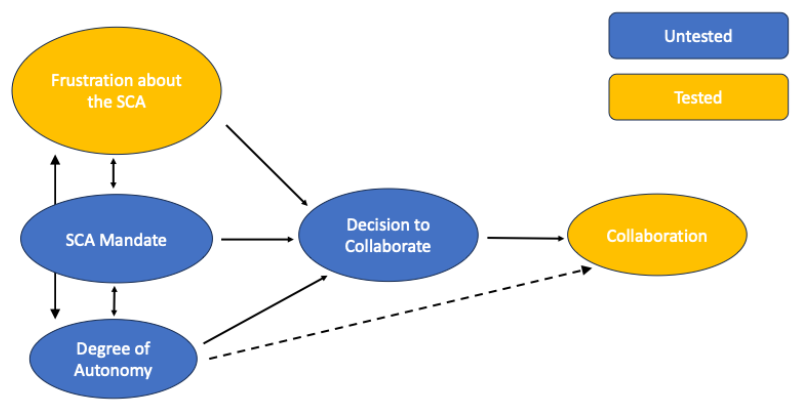
The Theory of Planned Behavior was identified as a theoretical foundation with the potential to explain the reported findings. Presuming rational actors, the theory suggests that behavior results from intentions formed by the influence of subjective perceptions about social norms, attitudes toward the behavior, and the individual's perceived control over it (Ajzen, 1985, 1991). In other words, societal attitudes, personal attitudes, and a person's perception of control all work together to influence whether a behavior occurs (Hardin-Fanning & Ricks, 2017). The diverse legislative landscape across the U.S. reflects a wide range of societal attitudes toward SOP for APRNs. This study’s findings begin to compile APRNs' attitudes regarding the law restricting Ohio APRN SOP, which most Ohio APRNs cannot effectively control, such as through choosing their collaborator. Theoretically, such data inform the understanding of how Ohio APRNs behave when collaborating with the regulated collaborating physician.
Figure 1. Theory of Planned Behavior model with the variables under study
Purpose
This study consisted of two phases. Phase one aimed to explore Ohio APRNs' reported frustrations at work. Once the most frequently reported frustration was identified, phase two began, where relationships between this frustration and other collected information were examined for relevance. Specifically, the most common work frustration (SCA law) was analyzed through the lens of the Theory of Planned Behavior to identify any links with subsequent behaviors, including the frequency of collaborative events with the regulated collaborating physician (Ajzen, 1985, 1991).
Methods
The Ohio Board of Nursing provided a list of 22,072 Ohio APRNs in response to the first author’s inquiry. After removing duplicates, all APRNs (n=21,842) were emailed an invitation to complete a survey. The emails were sent in batches over two weeks during spring 2022. Responses were received from 343 APRNs, resulting in a 1.6% response rate. However, 81 respondents were excluded due to missing data, reducing the sample to 262. Using G*Power 3.1.9.7 (Faul et al., 2007), an a priori power analysis was performed for point biserial correlation (the association between continuous frequency of collaboration and the binary presence or absence of high frustration). With alpha set at .05 and power of .8, detecting a small to moderate effect (r=.2) required 191 participants. With the final sample of 262 and alpha at .05, a posterior sensitivity analysis indicated an actual power of 0.909 (Cohen, 1992; Sullivan & Feinn, 2012; Ferguson, 2016).
The study authors created the survey and used Qualtrics for distribution and data collection. Exclusion criteria included non-active APRN status in Ohio. Consent was implied by voluntarily completing the survey. The Institutional Review Board at Ursuline College reviewed the study design and classified it as exempt. After the first author changed employment locations following data collection, Ursuline College and Ohio State University entered into a data use agreement. Survey questions are provided below.
Variables
First, respondents were asked whether they were active Ohio APRNs. Any respondents who answered no were automatically excluded from the rest of the survey. Those who answered yes were able to proceed. Next, respondents answered demographic questions about gender, age, and race. They selected a gender from the options: male, female, non-binary/third gender, and prefer not to answer, which was coded as a categorical variable. Respondents provided their age in years, coded as a continuous variable. They then identified their race from a list of mutually exclusive options: Caucasian, African American, Hispanic, and other. Race was coded as a categorical variable. Respondents also indicated their primary work geography (urban, rural, suburban). These options were not mutually exclusive, meaning more than one could be selected. Work geography was treated as a categorical variable. Finally, the respondents provided their years of APRN experience, a continuous variable.
Survey respondents were then asked about their clinical practice settings. The APRN respondents chose from several provided work setting options: primary care, pediatrics, psychiatry, women’s health, acute care, orthopedics, oncology, cardiology, and geriatrics. Again, these choices were not mutually exclusive. Work setting was treated as a categorical variable. During analysis (see below), work setting options were combined into primary care, acute care, psychiatry, and none of these to simplify the data.
Respondents were asked to rank five potential frustrations in practice as an Ohio APRN, selecting a unique position from one (least frustrating) to five (most frustrating). "Does not apply” was coded as six. The options provided included: "low pay,” “work hours,” “work volume,” “COVID concerns,” and “Ohio’s required SCA.” The first two authors, with twenty-eight years of combined APRN experience in Ohio, chose these stressors based on their anecdotal familiarity. Caution was taken regarding including respondents' frustration with the collaboration mandate in Ohio (represented by the choice "Ohio's required SCA") because it was uncertain how often this would be selected or if it might upset participants. Therefore, the team decided to hide this option among the others to reduce potential offense. Respondents were asked to rank five potential frustrations in practice...
The authors were also interested in how often collaborative events occurred but chose to ask about it directly. The question was: “On average, how many times per month have you collaborated with your physician collaborator (the specific physician who is identified in your SCA) in the past year?” This was treated as a continuous variable. The final questions asked whether respondents pay the physician identified in their SCA (yes/no) and how many years they plan to leave APRN practice in Ohio. Neither of these last two questions were used in subsequent analysis at this time.
Analysis Plan
After completing the survey, the data was checked for missing values. Once the final dataset was identified, descriptive statistics and frequency analyses were conducted. State-mandated collaboration was the most commonly selected frustration in phase one. Therefore, the authors used it as a variable of interest in phase two to explore relationships between this frustration and other collected data. The study found an inverse correlation between APRN respondents' frustration with the state mandate for collaboration and the frequency of collaborative events with the specific physician identified to Ohio as their collaborator.
Results
Sample
Responses were received from 343 APRNs. Listwise deletion for missing responses was performed for simplicity, resulting in the removal of 81 partial responses. Consequently, the final sample size decreased to 262.
Table 1. Respondent Characteristics
|
|
N |
Percentage |
Mean |
Standard Deviation |
|---|---|---|---|---|
|
Gender |
||||
|
Male |
22 |
8.4 |
|
|
|
Female |
239 |
91.2 |
|
|
|
Race |
||||
|
Caucasian |
246 |
93.9 |
|
|
|
Non-Caucasian |
16 |
6.1 |
|
|
|
Age |
|
|
54.4 |
9.57 |
|
Years of APRN Experience |
|
|
14.7 |
8.61 |
|
Work Geography |
||||
|
Urban |
126 |
48.1 |
|
|
|
Suburban |
101 |
38.5 |
|
|
|
Rural |
46 |
17.6 |
|
|
|
Work Setting |
||||
|
Primary Care |
98 |
37.4 |
|
|
|
Acute Care |
43 |
16.4 |
|
|
|
Psychiatry |
40 |
15.3 |
|
|
|
None of these |
92 |
35.1 |
|
|
Note. Work geography and work setting choices were not coded as mutually exclusive, thus their respective totals may not equal 100 percent.
Respondents were predominantly female (91.2%) and Caucasian (93.9%). They reported working in urban (48.1%), suburban (38.5%), and rural (17.6%) settings (choices not mutually exclusive). Respondents were older, with an average age of 54.4 years and a median of 55 years. APRN experience ranged from 1 to 39 years, with an average of 14.7 years (SD=8.61) and a median of 14 years. Respondents described their practice areas as primary care (37.4%), acute care (16.4%), psychiatry (15.3%), and none of these (35.1%). See Table 1 for a visual representation of respondent characteristics. The limited variation in variables such as “gender” and the collinearity among others, including experience, age, and work setting, restricted the ability to use multiple regression techniques to identify the effect of other factors that might contribute to frustration with the SCA.
Frustrations
Participants were asked to rank five common frustrations (compensation, work hours, work volume, coronavirus issues, SCA). They were to rate these frustrations on a scale where one indicates the least frustration and five the most. “Does not apply” was coded as six. Respondents were instructed to assign unique rankings to each frustration, with only one being ranked as a five, one as a four, and so on. Although this instruction was provided, not all respondents followed it.
Respondents rated low pay as a level five frustration 25.2% of the time (n=66). Work hours were ranked at a level five frustration 15.3% of the time (n=40). Work volume was considered a level five frustration by 22.9% of respondents (n=60). Only 17 respondents (6.5%) identified coronavirus concerns as their top frustration (level five).
The most frustrating option for the majority of respondents was the SCA (40.1%; n=105). One hundred fifty respondents (57.3% of this group) rated the SCA as among the top two frustration levels (four or five). For further analysis, the authors classified any respondent who assigned the SCA a four or five as "highly frustrated.” High levels of frustration were significantly and directly linked to both APRN experience (r=.161, p<.01) and age (r=.151, p<.05).
Level of Collaboration
Collaborative events between the APRN and the SCA-specific physician were measured as a continuous variable. Respondents provided an estimated number of collaborative events per month, ranging from none to multiple times a day. The authors conceptualized the range as zero to twenty or more, defining twenty interactions as daily contact based on a four-week month and a five-day workweek.
Overall, the average number of monthly collaborative events was low. Sixty-three respondents (24%) reported no monthly collaboration with the physician identified in their SCAs. Seventy-seven respondents (29.4%) reported a collaborative event frequency of less than once per month. Nearly half of the respondents (46.6%; n=122) reported one or fewer collaborative events per month. The average number of events was 5.84 hours per month (SD=12.06), with a median of two hours per month. The average is notably higher than the median due to the wide variation in frequency (0-20 or more collaborative events per month). The practice setting likely influences these results; 9.2% of APRN respondents report daily or multiple daily interactions, possibly because they work in a shared practice setting alongside their physician colleagues.
SCA Collaboration and SCA Frustration
The study examined the correlation between highly frustrated APRNs and their frequency of collaborative events using point biserial correlation. The goal was to analyze the relationship between a continuous variable (hours of collaborative events per month) and a dichotomous variable (highly frustrated with SCA or not). The analysis showed a statistically significant inverse correlation of small to moderate size (r = -.161; p = .009). In simple terms, high frustration with the SCA is significantly linked to fewer monthly collaborative events in this sample.
Discussion
The results show that, despite the expected frustration caused by coronavirus concerns, most respondents are highly frustrated with Ohio’s mandated collaboration law, or SCA. Additionally, the legally required collaboration between APRNs and collaborating physicians varies greatly in how often it occurs among this group of respondents. While a minority of respondents work with their assigned physician daily or more often, most do so rarely. In fact, many respondents report no collaborative interactions with the physician assigned through their SCA.
Although empirically ambiguous, these results can be interpreted using theory. From the perspective of The Theory of Planned Behavior, one of the most tested models for understanding reasoned actions, the directionality between variables is implied. The Theory of Planned Behavior argues that behavior stems from intentions shaped by attitudes, perceptions of social norms, and perceived control over the behavior (Ajzen, 1985, 1991). Guided by this theory, the authors hypothesize that, in a regulatory mandate lacking a clear clinical need, APRN attitudes toward the SCA will influence collaborative behavior with the mandated physician. Specifically, they suggest that negative beliefs decrease intention and lead to less collaboration (see Figure 1). This means that the frustration with the SCA shown in the data predicts fewer collaborative events.
This data reflects the initial survey of Ohio APRNs' frustration with a state environment that limits their SOP. Although little is known about individual provider attitudes toward SOP restrictions and full practice rights for APRNs, the context of these results speaks loudly. Decades of consistent patient outcome data show no significant difference between care provided by a physician and an NP (Geller & Swan, 2021). Additionally, analyzing NPs' patient safety outcomes across different SOP environments has not revealed notable differences between less and more restrictive states (Geller & Swan, 2021). In other words, “state regulations restricting NP scope of practice do not improve the quality of care” (Perloff et al., 2019, p. 597). Other efforts to link restrictive SOPs with patient benefits have also failed to show positive results (Smith, 2021). Furthermore, there is evidence that an NP's organizational climate influences the quality of care; specifically, higher scores on the Nurse Practitioner Primary Care Organizational Climate Questionnaire's "Independent Practice and Support" subscale are associated with a 60% increase in quality care measures related to patients’ cholesterol testing in a large Massachusetts study (Poghosyan et al., 2018). The Federal Trade Commission also stated in 2014 that state mandates restricting APRN practice by physicians violate antitrust law (Gilman et al., 2014). Considering all this information, it’s less surprising that our respondents expressed stronger frustration with Ohio's SCA law than with other issues.
Implications
This study provides an important initial look at APRN attitudes toward the legally mandated SCA in Ohio. High frustration levels with the SCA were inversely associated with collaboration with the physician specified in the SCA. Although we lack empirical evidence on the direction of this relationship, the pathway for future research is clear. Additional studies could explore predictors of frustration with the SCA and identify specific enablers of the SCA law in Ohio.
If, as theoretically modeled, Ohio’s SCA legal mandate exists without evidence of benefit to patient care, frustrates the majority of Ohio APRNs, and potentially reduces the likelihood of APRN-physician collaboration, it is reasonable to examine its value. Considering that state-mandated collaborative agreements tend to increase healthcare costs (Gilman et al., 2014; Ritter et al., 2018), further review is fiscally necessary. Additionally, since such agreements often limit access to care (Gilman et al., 2014; Martin & Alexander, 2019), this warrants moral consideration for Ohio’s patients. Nurses have an ethical duty to advocate for patient care through an emancipatory lens (Chinn et al., 2022). If most of Ohio’s APRNs are frustrated with current laws governing practice, they should voice their concerns to their state legislators regularly. Moreover, open discussion of workplace frustrations is essential for mobilizing nurses and enacting change. Advocating for reasonable work environments is a fundamental and necessary step toward effective patient advocacy.
Members of the Ohio Association of Advanced Practice Nurses (OAAPN) have repeatedly introduced legislation to stop or significantly change SCA laws since the group’s founding in 1996 (OAAPN, 2021). However, the SCA law remains in effect. APRNs frustrated with this law might benefit from continuing and persisting with these legislative efforts. Researchers should examine past lobbying failures. Educators are encouraged to involve future APRNs in discussions about state-mandated collaboration, thereby enhancing their understanding and advocacy skills.
Limitations
Our findings should be considered in light of the study's limitations. Our respondent sample lacked diversity to better understand differences in race and gender. Equally important, we should have surveyed with greater specificity to fully grasp distinctions in APRN practice settings and levels of independence. Additionally, the data from our cross-sectional survey has inherent limitations in predicting future outcomes. Besides the Theory of Planned Behavior, we currently lack a methodological basis for assuming the direction of the relationship between frustration and collaboration.
However, the results of this study provide guidance for future research. Additional studies are needed to conduct predictive analyses of the relationships between the variables examined. The insights gained from such research can contribute to improved public policy in the healthcare sector. Refining the data collected to address questions raised by the current study will be crucial for advancing this research, which is especially urgent given Ohio's healthcare landscape for the reasons outlined above. Such further research will help identify causal relationships among characteristics and better inform policymakers affecting the professional lives of APRNs in Ohio. Furthermore, as we all learned in 2020, the health and safety of the general population heavily depend on these issues.
Conclusion
The findings of this study highlight the important role that regulatory environments can play in shaping the professional experiences of APRNs in Ohio. Among surveyed APRNs, frustration with the state-mandated standard care arrangement was the most commonly reported workplace frustration and was significantly linked to decreased collaboration with the designated physician collaborator. These results suggest that policies designed to structure collaborative practice may not always foster meaningful professional interaction and might instead lead to provider dissatisfaction. While more research is needed to better understand causal relationships and broader implications, these findings add to ongoing discussions about APRN scope of practice, workforce satisfaction, and healthcare access. Continued research, policy review, and professional advocacy will be crucial to ensure that regulatory frameworks support both effective collaboration and the optimal use of the APRN workforce.
Authors
Morgan Wiggins, DNP, APRN, PMHNP-BC
Email: wiggins.213@osu.edu
ORCID ID: 0000-0003-3336-0144
Morgan Wiggins, DNP, APRN, PMHNP-BC received her BSN from Cleveland State University in 2005. She received her MSN and became a psychiatric mental health nurse practitioner from Kent State University in 2010. She received her DNP from Case Western Reserve University in 2021. She began teaching future psychiatric nurse practitioners full-time in 2020. Dr. Wiggins is a Clinical Assistant Professor of Practice at The Ohio State University College of Nursing, Columbus, OH, USA
Dr. Elizabeth Carroll, DNP, APRN, PMHNP-BC
Email: liz@hudsonbh.com
Dr. Elizabeth Carroll, DNP, APRN, PMHNP-BC, is an Assistant Professor of Nursing at Ursuline College, Pepper Pike, OH, USA. Dr. Carroll received her BSN from the College of Mount Saint Vincent in 1996. She received her MSN and became a psychiatric mental health nurse practitioner from Kent State University in 2011. She received her DNP from Ursuline College in 2023. She began teaching future psychiatric nurse practitioners full-time in 2021.
Rosemarie Emanuele, PhD
Email: remanuele@ursuline.edu
Rosemarie Emanuele, PhD, is a Professor of Economics at Ursuline College, Pepper Pike, OH, USA. Dr. Emanuele has a bachelor’s degree in economics from Georgetown University and a PhD in economics from Boston College. She is primarily a labor economist focusing on public-sector economics. Additional research interests include health economics and the relationship between law and economics. She teaches various mathematics and economics courses to undergraduate students.
References
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & Beckmann, J. (Eds.), Action control: From cognition to behavior (pp. 11-39). Springer-Verlag. https://doi.org/10.1007/978-3-642-69746-3_2
Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179-211.
AANP. (2022, Oct). State Practice Environment. AANP. Retrieved 6/8/2023 from https://www.aanp.org/advocacy/state/state-practice-environment
ANA. (2017, Mar 9). A Look at Each APRN Role. ANA. Retrieved 7/17/2024 from https://www.myamericannurse.com/look-aprn-role
ANA. (2017, Oct 19). Advanced Practice Registered Nurse (APRN).ANA. Retrieved 6/8/2023 from https://www.nursingworld.org/practice-policy/workforce/what-is-nursing/aprn/
ANA. (2017, Oct 20). State Law and Regulation. ANA. Retrieved 7/17/2023 from https://www.nursingworld.org/practice-policy/state-law-and-regulation/
Barnett, M., Balkissoon, C., & Sandhu, J. (2021). The level of quality care nurse practitioners provide compared with their physician colleagues in the primary care setting: A systematic review. Journal of the American Association of Nurse Practitioners, 34(3), 457-464. https://doi.org/10.1097/JXX.0000000000000660
Chinn, P.L., Kramer, M.K., & Sitzman, K. (2022). Knowledge development in nursing: Theory and Process (11th edition). Elsevier.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155-159. https://doi.org/10.1037/0033-2909.112.1.155
Davis, M. (2022, Aug 22). Health Insurance: Amid a Physician Shortage, 51% of Primary Care Providers Are Nurse Practitioners and Physician Assistants. Value Penguin by LendingTree. Retrieved 8/2/2023 from https://www.valuepenguin.com/primary-care-providers-study
Everett, C.M., Morgan, P., Smith, V.A., Woolson, S., Edelman, D., Hendrix, C.C., Berkowitz,T., White, B., & Jackson, G.L. (2019). Primary care provider type: Are there differences in patients’ intermediate diabetes outcomes? Journal of the American Academy of Physician Assistants, 32(6), 36-42. https://doi.org/10.1097/01.jaa.0000558239.06875.0b
Faul, F., Erdfelder, E., Lang, A-G., & Buchner, A. (2007). G*Power 3: A flexible statisticalpower analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175-191.
Ferguson, C.J. (2016). An effect size primer: A guide for clinicians and researchers. In A.E.
Kazdin (Ed.), Methodological issues & strategies in clinical research: Fourth edition (pp.301-310). American Psychological Association. https://doi.org/10.1037/14805-020
Geller, D. & Swan, B. A. (2021). Recent evidence of nurse practitioner outcomes in a variety ofcare settings. Journal of the American Association of Nurse Practitioners 33(10), 771-1 https://doi.org/10.1097/JXX.0000000000000451
Gilman, J.J., Koslov, T.I., Feinstein, D.L., Gaynor, M., Bloom, M.J., Hertzendork, M.N., Hilder, E.R., Schmidt, D.R., & Schultheiss, P. (2014). Policy perspectives: Competition advocacy and the regulation of advanced practice nurse practitioners. Federal TradeCommission. www.ftc.gov/policy/reports/policy-reports/commission-and-staff-reports
Hardin-Fanning, F. & Ricks, J.M. (2017). Attitudes, social norms, and perceived behavioralcontrol factors influencing participation in a cooking skills program in rural CentralAppalachia. Global Health Promotion, 24(4), 43-52. https://doi.org/10.1177/1757975916636792
Htay, M., & Whitehead, D. (2021). The effectiveness of the role of advanced nurse practitionerscompared to physician-led or usual care: A systematic review. International Journal of Nursing Studies Advances, 3, 100034. https://doi.org/10.1016/j.ijnsa.2021.100034
Jackson, G.L., Smith, V.A., Edelman, D., Woolson, S.L., Hendrix, C.C., Everett, C.M.,Berkowitz, T.S., White, B.S., & Morgan, P.A. (2018). Intermediate diabetes outcomes inpatients managed by physicians, nurse practitioners, or physician assistants: A cohortstudy. Annals of Internal Medicine, 169, 825-835. https://doi.org/10.7326/M17-1987
Jiao, S., Murimi, I.B., Stafford, R.S., Mojtabai, R., & Alexander, G.C. (2018). Quality ofprescribing by physicians, nurse practitioners, and physician assistants in the UnitedStates. Pharmacotherapy, 38(4), 417-427. https://doi.org/10.1002/phar.2095
Kraus, E. & DuBois, J.M. (2016). Knowing your limits: A qualitative study of physician andnurse practitioner perspectives on NP independence in primary care. Journal of General Internal Medicine, 32(3), 284-290. https://doi.org/10.1007/s11606-016-3896-7
Laurant, M., van der Biezen, M., Wijers, N., Watananirun, K., Kontopantelis, E., & van Vught, A.J.A.H. (2018). Nurses as substitutes for doctors in primary care. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.cd001271.pub3
Martin, B. & Alexander, M. (2019). The economic burden and practice restrictions associated with collaborative practice agreements: A national survey of advanced practice registered nurses. Journal of Nursing Regulation, 9(4), 22-30.
Martsolf, G.R., Auerbach, D.I., & Arifkhanova, A. (2015). The Impact of Full Practice Authority for Nurse Practitioners and Other Advanced Practice Registered Nurses in Ohio (RR-848-OAAPN). Rand Corporation. https://www.rand.org/pubs/research_reports/RR848.html
National Academies of Sciences, Engineering, and Medicine. (2021). The future of nursing 2020-2030: Charting a path to achieve health equity. The National Academies Press. http://nap.nationalacademies.org/25982
Ohio Association of Advanced Practice Nurses. (2021, Mar 22). Our Accomplishments and Legislative Efforts. Ohio Association of Advanced Practice Nurses. Retrieved 9/27/24 from https://oaapn.org/2021/03/our-accomplishments-and-legislative-efforts/
Ohio Association of Advanced Practice Nurses. (2023, Jan 20). Standard Care Agreement.
Ohio Association of Advanced Practice Nurses. Retrieved 6/8/2023 from https://oaapn.org/regulation/standard-care-arrangement/
Ohio Board of Nursing. (no date). Advanced Practice Registered Nurse 2021 Ohio workforce data summary report. Retrieved 7/17/2023 from https://nursing.ohio.gov/static/uploads /2022/07/APRN-Workforce-Data-Report_final.pdf
O'Reilly-Jacob, M., Zwilling, J., Perloff, J., Freeman, P., Brown, E., Donelan, K. (2023). Earlyimplementation of full-practice authority: A survey of Massachusetts nurse practitioners.Journal of the American Association of Nurse Practitioners 35(4), 235-241. https://doi.org/10.1097/JXX.0000000000000853
Perloff, J., Clarke, S., DesRoches, C.M., O’Reilly-Jacob, M. & Buerhaus, P. (2019). Associationof state-level restrictions in nurse practitioner scope of practice with the quality ofprimary care provided to Medicare beneficiaries. Medical Care Research and Review, 76(5), 597-626. https://doi.org/10.1177/1077558717732402
Poghosyan, L., Norful, A.A., Liu, J., Friedberg, M.W. (2018). Nurse practitioner practiceenvironments in primary care and quality of care for chronic diseases. Medical Care, 56(9), 791-797. https://doi.org/10.1097/MLR.0000000000000961
Ritter, A.Z., Bowles, K.H., O’Sullivan, A.L., Carthon, M.B., & Fairman, J.A. (2018). A policy analysis of legally required supervision of nurse practitioners and other health professionals. Nursing Outlook, 66(6), 551-559. https://doi.org/10.1016/j.outlook.2018.05.004
Rule 4723-8-01 Definitions, Ohio Administrative Code, (2/1/2021). https://codes.ohio.gov/ohio-administrative-code/rule-4723-8-01
Rule 4723-8-04 Standard care arrangement for a certified nurse-midwife, certified nurse practitioner, and clinical nurse specialist, Ohio Administrative Code, (2/1/2022). https://codes.ohio.gov/ohio-administrative-code/rule-4723-8-04
Ruth, K., Myers, C.R., Likes, W., Schorn, M.N. (2022). Breaking down institutional barriers toadvanced practice registered nurse practice. Nursing Administration Quarterly, 46(2),137-143. https://doi.org/10.1097/NAQ.0000000000000518
Smith, L. B. (2021). The effect of nurse practitioner scope of practice laws on primary care delivery. Health Economics, 31(1), 21-41. https://doi.org/10.1002/hec.4438
Sullivan, G.M. & Feinn, R. (2012). Using effect size—or why the p value is not enough. Journal of Graduate Medical Education, 4(3), 279-282. https://doi.org/10.4300/JGME-D-12-00156.1
Yang, Y., Long, Q., Jackson, S.L., Rhee, M.K., Tomolo, A., Olson, D., & Phillips, L.S. (2017).Nurse practitioners, physician assistants, and physicians are comparable in managing thefirst five years of diabetes. The American Journal of Medicine, 131(3), 276-283. https://doi.org/10.1016/j.amjmed.2017.08.026
Zhang, P. & Patel, P. (2022, Sept 19). Practitioners and Prescriptive Authority. StatPearls.Retrieved 7/8/2023 from https://www.ncbi.nlm.nih.gov/books/NBK574557/
