


The exponential rise in the number of older adults suggests a growing need for geriatricians. Up to 30,000 geriatricians will be needed in the United States by 2030 to care for this aging population and physician supply will be unable to keep up with demand. A potential solution to this shortage could be the addition of advanced practice clinicians within the geriatric specialty. In 2022, a Department of Veterans Affairs (VA) site created a geriatrics nurse practitioner residency program. The residency offers a one-year immersive geriatric clinical experience for new graduate nurse practitioners. Didactic content is an important supplement to clinical education and focuses on topics specific to our patient population, allowing the residents to tailor their care to the needs of patients. This article describes the background, development, and implementation of a geriatrics nurse practitioner residency program, an analysis of the first year program outcomes, and concludes with implications for practice.
Key Words: nurse practitioner residency, nurse practitioner fellowship, post-graduate nurse practitioner training
With this exponential rise in the number of older adults comes a growing need for geriatricians.Between 2010 and 2020 the number of adults in the United States (US) aged 65 and older experienced the most substantial growth in any decade since 1880 to 1890 (Caplan & Rabe, 2023). Further, given the aging “baby boomer” population, born between approximately 1946 and 1964, it is anticipated that this share of older adults will only continue to grow. Estimated projections are that older adults will comprise 21% of the population by 2030 (Vespa, 2018). With this exponential rise in the number of older adults comes a growing need for geriatricians. Estimates are that 30,000 geriatricians will be needed in the United States by 2030 to care for the aging population and that physician supply will be unable to meet this demand. For context, there were 7,428 certified geriatricians in 2014 (Span, 2020).
A potential solution to this shortage could be the addition of advanced practice clinicians within the geriatric specialty.A potential solution to this shortage could be the addition of advanced practice clinicians within the geriatric specialty. More than 36,000 nurse practitioners graduated in 2020-2021 (American Association of Nurse Practitioners [AANP], 2023). Currently, 83.2% of full-time nurse practitioners already treat patients on Medicare (AANP, 2023). However, within this vast pool of clinicians is an important need to ensure they are adequately prepared with expertise in the care of the complex geriatric patient. Nurse practitioners who hold certifications in adult-gerontology, adult, family, or gerontology may all work in geriatric care settings. A key question is then: “How do we ensure that new nurse practitioners, from a variety of training programs, are provided with tools and skills to become competent and confident providers in a specialty that requires multi-faceted, comprehensive care?”
In 2022, a Department of Veterans Affairs (VA) site implemented a geriatrics nurse practitioner (NP) residency program. Fully sponsored by the VA Office of Academic Affiliations, the residency offers a one-year immersive geriatric clinical experience for new graduate nurse practitioners which includes dedicated time for learning of didactic content. This article describes the background, development, and implementation of the geriatrics nurse practitioner residency program, an analysis of the first year program outcomes, and concludes with implications for practice.
Background
In 2011, the Institute of Medicine (IOM) published the report, The Future of Nursing, Leading Change, Advancing Health with recommendations for implementation of nurse practitioner residency programs following graduation and/or when changing area of practice (Committee on the Robert Wood Johnson, 2011). The IOM committee members argued that substantial support should be given to put residency initiatives into practice.
...studies have shown that NP residency training has a positive impact on job satisfaction...In the time that has passed since the IOM report (Committee on the Robert Wood Johnson, 2011) was published over 75 facilities in a variety of care settings, including the VA, have implemented nurse practitioner residency and fellowship programs (Meissen, 2019). Proponents have found that these residency programs offer an opportunity beyond required NP education and training. Faraz (2019) concluded that mentorship, meaningful work, role clarity, and work-life balance were important factors to successful transition to practice. In a workforce of nurses challenged by turnover and burnout, retention and job satisfaction can be important considerations. To date, studies have shown that NP residency training has a positive impact on job satisfaction and accelerates the learning curve related to the role’s requirements (Bryant & Parker, 2019; Pleshkan & Hussey, 2020).
In 2022, cognizant of the need to develop confident and competent new graduate nurse practitioners, a Department of Veterans Affairs site implemented a geriatrics and extended care nurse practitioner residency (GEC-NPR) program. The VA is a department within the United States government responsible for the care of the nation’s military veterans. Included within this department are over 150 medical centers and clinics across the nation. The VA Office of Academic Affiliations (OAA) recognizes the importance of NP residency programs and provides program sponsorship, guidance, support, and funding. Acknowledging the specific health conditions and needs of the veteran population, the GEC-NPR is tailored to provide education about topics related to geriatric care, veteran-specific conditions, and how these may intertwine with the broader plan of care for patients.
The Nurse Practitioner Residency Program
Mission, Goals, and Objectives The mission of the GEC-NPR program at the VA is to build upon the foundational knowledge of new graduates to develop competent and confident nurse practitioners, equipped with the geriatric-specific knowledge and skills necessary to care for the specific needs of veterans within the VA and the community. This program also aims to improve recruitment and retention efforts of the VA by providing a consistent stream of well-trained nurse practitioners for the workforce.
The goals and objectives of the program are to: 1) Improve clinical skills, confidence, and productivity of nurse practitioner residents through comprehensive clinical and didactic training experiences; 2) Provide access to quality care for veterans through the recruitment and retention of nurse practitioner resident program graduates; 3) Promote interprofessional collaboration through clinical care and educational opportunities; 4) Exhibit the skills necessary to provide veteran-centric, high-quality care, and 5) Prepare nurse practitioner residents to provide care in a variety of settings within the VA.
Recruitment, Qualifications, and Selection of Nurse Practitioner Residents Nurse practitioners are recruited for the GEC-NPR through VA nurse recruiters, emails, and flyers to schools in the region, in addition to presentations to local graduate programs. Additionally, information about the program in the application process can be found on our webpage (U.S. Department of VA, 2024). Candidates must meet a set of clearly defined facility and program requirements and are required to submit a standard application for consideration. Each program year, a team of clinical faculty reviews applications and conducts interviews with finalists. The panel ultimately selects up to three residents for the program annually. Applicants may be tentatively selected pending completion of educational or certification/licensure requirements but cannot be hired to begin the program until all requirements are met.
Program Structure The year-long VA residency builds upon standard competencies for nurse practitioners to improve knowledge and skills with a focus on geriatric-specific competencies and age-friendly care. The program is dedicated to a geriatric and interprofessional focus for both experiential and didactic learning opportunities. Nurse practitioner residents spend the majority of their clinical time in core longitudinal experiences in outpatient geriatrics clinic, subacute rehabilitation, and long-term care. They also participate in short-term rotations in areas such as hospice and palliative care, pain management, speech and language pathology, women’s health, and home-based primary care. These rotations are determined based upon individual learning needs of the residents, preferences for clinical rotations and professional interest, and space/preceptor availability within the VA facility.
The program is dedicated to a geriatric and interprofessional focus for both experiential and didactic learning opportunities.The Community Living Center (CLC) at the program site serves as the primary location for the NP residency program. The center is an 87-bed facility, focused on subacute rehabilitation and long-term care for the geriatric population. The core/primary team consists of an attending physician, NP, and NP resident. Within the CLC, the NP resident team is expected to cover anywhere from 10 to 12 patients at a given time. Residents follow their patients from the time of admission; they coordinate interprofessional care throughout their stay and facilitate discharge planning and care transition to the outpatient setting. The broader interdisciplinary team within the CLC includes dietitians; speech and language pathologists; physical, occupational, and recreational therapists; and mental health professionals. Nurse practitioner residents are expected to work with the entire team to provide optimal care and coordinated services.
The geriatrics outpatient continuity clinic is located on the same campus. This clinic allows for longitudinal outpatient care throughout the program year, with a focus on care of the complex geriatric patient. In addition, NP residents participate in the ‘Matters Most’ clinic, which is focused on aligning what matters most to the patient, taking into consideration health, wellness, and overarching goals.
...NP residents participate in the ‘Matters Most’ clinic, which is focused on aligning what matters most to the patient...Within each clinical site, the NP residents work with patients to develop a plan of care that incorporates the varying values, desires, and beliefs of each individual veteran. Residents work with preceptors to refine this skill over time, and to develop rapport with those patients whom they see on a longitudinal basis.
Progression Model The GEC-NPR has a three-level, time-bound progression model. NP residents spend 80% of their time on clinical activities, and 20% on didactic content throughout the program year. Progression model level I consists of orientation to VA processes, programs, and facilities, and transitions into building foundational knowledge. Residents receive a comprehensive orientation to prepare them to start clinical practice as they begin to experience the ever-changing healthcare environment. Residents determine areas of clinical need and desire. The beginning of clinical rotations requires recall of basic concepts, and the use of clinical reasoning skills are put in practice.
Level II of the model focuses on beginning to understand VA processes, programs, and facilities in relation to clinical care. Residents have graduated levels of responsibility for patient care. They incorporate required didactic content to solidify clinical reasoning by applying this information in real time clinical practice. Residents learn to make decisions more independently. They can explore elective clinical opportunities to broaden their clinical knowledge and increase exposure to diverse areas of practice. Residents display an understanding of pathophysiology and pharmacology and analyze evidence-based treatment guidelines in their decision-making and treatment plans.
Model level III requires NP residents to demonstrate proficient veteran-centric care while navigating the complex challenges of translating rapidly expanding knowledge into practice. The processes, programs, and facilities at the VA become easier to differentiate, and a solid set of practice resources have developed, along with strong mentorship from colleagues, preceptors, program directors, and others. In level III, residents continue to assume graduated levels of responsibility. They are able to evaluate their own practice, defend practice decisions, and justify the philosophy of care they choose to define their own practice as they transition into the role of an independent, competent, and confident provider.
Didactic Content and Required Projects During the residency year, NP residents have flexibility to engage in a variety of didactic interprofessional learning experiences. On average, residents are expected to participate in eight hours of didactic learning experiences each week. Didactic content is an important supplement to clinical education and focuses on topics specific to our patient population, allowing residents to tailor their care to the needs of their patients. These experiences can include, but are not limited to, guest speaker presentations, case conferences, grand rounds, clinical simulation activities, journal clubs, or work toward a required evidence-based practice (EBP) or quality improvement (QI) project.
During the residency year, NP residents have flexibility to engage in a variety of didactic interprofessional learning experiences.Early in the residency program, each NP resident works with the team to select a potential QI or EBP project of interest to be completed within the facility, in collaboration with faculty through our academic partnership. Residents assess the problem, formulate a project question, conduct a thorough literature search, critically appraise the literature, and evaluate the evidence. They formulate and propose a plan to address the problem by collaborating with the interprofessional team members described above. Residents are encouraged to work closely with faculty, mentors, and their program director (PD) to disseminate their scholarly work through podium or poster presentations at national scientific meetings, and/or manuscript submissions.
Program Evaluation
Nurse practitioner residents and program faculty complete evaluations in accordance with VA Office of Academic Affiliations requirements to assess resident performance. These evaluations are completed at regular intervals throughout the year as outlined in the Table. In part, this includes a self and faculty rated competency self-assessments; a self-assessment of confidence in the performance of core clinical skills and abilities; and an overall satisfaction with the GEC-NPR program. Additionally, the program director completes an evaluation of organizational impact and overall program outcomes (e.g., data for recruitment, job placement, retention, and turnover of residents hired by the VA). These data are reviewed and disseminated in a comprehensive annual program report.
Table. Program Evaluations
|
Evaluation Instrument |
Time Frame |
|---|---|
|
Resident Competency Self-Assessment |
Baseline, 6 months and 12 months |
|
Faculty Rated Competency Assessment |
Baseline, 6 months and 12 months |
|
Resident Confidence in Practice Assessment |
Baseline, 6 months and 12 months |
|
Trainee Satisfaction Survey |
Completion of Program (12 months) |
Program Outcomes and Organizational Retention
Trainee Satisfaction. The inaugural cohort in the GEC-NPR program from academic year 2022-2023 reported the top three reasons for choosing an NP residency as: 1) to gain additional knowledge and skills to transition into a professional role; 2) to build confidence to practice in a challenging clinical setting; and 3) to work towards future job opportunities within the VA. Program participants reported the highest level of satisfaction (i.e., very satisfied) within all assessed categories: clinical faculty/preceptors, clinical learning environment (e.g., number and diversity of patients seen, spectrum of patient problems, time), physical environment (e.g., workspace), VA working environment (e.g., welcoming/supportive environment), and overall satisfaction with the training experience.
The longitudinal experiences...were reported as the most helpful rotations for resident learning needs.Pre-program participant learning goals were to improve skills, and to become more comfortable in the NP role related to diagnosis and treatment of a variety of medical conditions. The longitudinal experiences (i.e., the geriatric continuity clinic, and CLC long-term care and subacute rehabilitation units) were reported as the most helpful rotations for resident learning needs. One resident reported that learning the VA processes and the various programs the VA offers was overwhelming and recommended more intensive training on VA computer systems at the beginning of the program.
Competency Assessment. Nurse practitioner resident self-perceived competency experienced the largest overall improvement over the program year in the domains of resource utilization (140%), health delivery system (106%), clinical leadership (100%), and quality improvement and evidence (100%) within the general core competencies (see Figure 1). Stress management and professional roles and responsibilities achieved more improvement over the second half of the year; however, these competencies were amongst the lowest scores in percent change and overall improvement given their initial high ratings. Conversely, the areas of informatics and technology, and ethical decision-making achieved the most improvement over the first half of the program.
Within the domain of geriatrics-specific competencies, the largest overall growth over the program year occurred in treatment (120%), diagnosis (106%), and knowledge of gerontological conditions and healthcare issues (95%). Patient and family education, follow-up and evaluation of the patient status, treatment, diagnosis, and assessment achieved more rapid growth over the first half of the program. Military/veteran-centric care, cultural knowledge, and knowledge of geriatric screening and assessment attained more improvement over the second half of the program year.
Figure 1. Nurse Practitioner Resident Perceived Competence Over a 12 Month Period
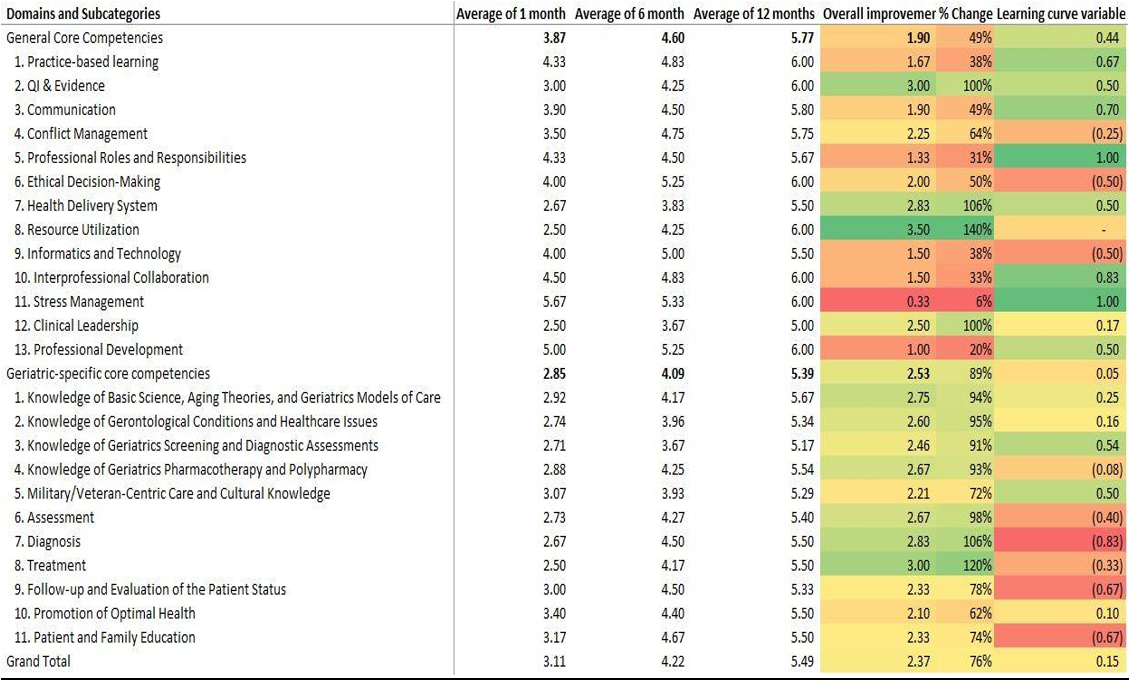
Note: Results in Figure 1 represent the average percent improvement in scores across time for questions related to competence of the NP resident, from their perspective. Likert scale responses range from 1 (critical deficiencies) to 6 (competent).
The faculty assessment of resident competency was assessed by evaluating the overarching domains and revealed the largest overall growth and percent change in competency in the domain of geriatric-specific core competencies (48%; see Figure 2). However, it should be noted that the domain of general core competency also achieved growth (32%), resulting in an overall improvement in assessed competence of 44% over the program year.
Figure 2. Faculty-Rated Nurse Practitioner Resident Competence Over a 12 Month Period
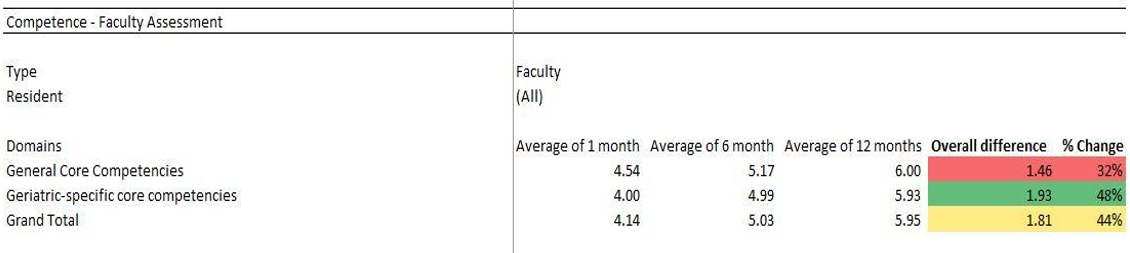
Note: Results in Figure 2 represent the average percent improvement in scores across time for questions related to competence of the resident, from the preceptor’s perspective. Likert scale responses range from 1 (critical deficiencies) to 6 (competent).
Confidence in Practice. The analysis of the resident self-perceived confidence in practice evaluation showed growth in confidence in all three areas assessed (see Figure 3): patient care (91%), communication (82%), and professional role (69%). Patient care achieved the highest amount of growth, as well as the largest change over time. An overall increase in confidence of 85% was achieved over the program year.
Figure 3. Nurse Practitioner Resident Self-Perceived Confidence in Practice
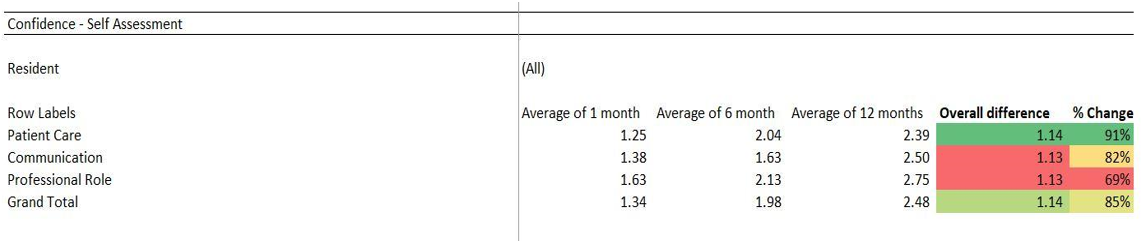
Note: Results in Figure 3 represent the average percent improvement in scores across time for questions related to confidence of the resident, from the resident’s perspective. Scale responses range from 0 (no confidence) to 6 (complete confidence).
Retention. Both graduates from the inaugural cohort were hired within the local VA healthcare system. As such this resulted in a 100% retention rate of those who graduated from the program during the time period for this evaluation.
Implications for Practice and Research
...longitudinal data on retention outcomes of program graduates will provide further insight into the cost-benefit of continuing NP residency programs.As we move into our second program year, there is ample opportunity to reflect on program successes, as well as areas for improvement. While our initial cohort achieved optimal organizational retention, and evaluation outcomes were largely positive, there are opportunities to further refine the program and amplify its impact.
Thus far, program outcomes related to competency and confidence in practice for new graduate NPs, as well as recruitment and retention, were all positive. Based on available data, more emphasis and didactic content focus on areas with low growth over the first half of the program year may provide additional benefit to program participants. These areas included military/veteran centered care, cultural knowledge, and knowledge of geriatric screening and assessment. Less didactic emphasis on areas of rapid immediate growth may provide less redundancy (e.g., patient and family education, treatment, and diagnosis). It is likely that continued education and practice in all of these domains correlate with increased confidence in practice.
...confidence and competence in practice of complex geriatric care were key markers of success...Further research is needed to investigate factors that may facilitate or hinder entry of NPs into a residency program, as well as the specific components of program didactic content and clinical structure that make a residency most successful related to competence and confidence in practice. Additionally, longitudinal data on retention outcomes of program graduates will provide further insight into the cost-benefit of continuing NP residency programs. It is imperative that organizations continue to provide published reviews of NP residency programs to both disseminate evidence of successful outcomes to support their existence and offer considerations for the refinement and optimization of program components.
Conclusion
Geriatrics NP residency programs may offer a steady workstream of clinicians who can contribute to a specialty in significant need.The results of our program evaluation offer current evidence of the positive outcomes of NP residency programs. Specifically, confidence and competence in practice of complex geriatric care were key markers of success for the GEC-NPR program. The results of this program evaluation lend an opportunity for continuous improvement at this VA practice site, as well as potential tools for success within new and existing nurse practitioner residencies.
Geriatrics NP residency programs may offer a steady workstream of clinicians who can contribute to a specialty in significant need. Such programs provide a promising avenue to provide the tools and skills to become confident and competent clinicians. The basic structure of the GEC-NPR program developed by the VA can be easily applied to specialties outside of geriatrics. We must look beyond debating the necessity of nurse practitioner residency programs, as the future depicted in the IOM (2011) report is now.
Authors
Alyssa Moore, DNP, APRN, NP-C
Email: alyssa.moore350@gmail.com
ORCID ID: 0009-0000-8806-2465
Alyssa Moore is a nurse practitioner, and recently served as Director of the Geriatrics Nurse Practitioner Residency Program at VA Boston. She holds board certification as a family nurse practitioner and has extensive clinical practice experience in adult and geriatric medicine. She received a BSN from South Dakota State University, an MSN from the University of Nevada, Las Vegas, and a DNP from Touro University Nevada. Nurse practitioner residency was a primary area of focus throughout her doctoral program, which has heavily influenced her desire to continually advocate for the advancement of high-quality residency training for new graduate nurse practitioners.
Sarah King, MD
Email: Sarah.King2@va.gov
ORCID ID: 0009-0007-2717-0869
Sarah King is a geriatrician at the VA Boston Healthcare System and is an Assistant Professor of Medicine at Boston University Chobanian & Avedisian School of Medicine. She completed medical school at the University of Vermont College of Medicine and completed internal medicine residency and geriatrics fellowship training at the Boston University Medical Center. She currently serves as Associate Program Director in the Geriatrics and Extended Care Nurse Practitioner Residency at VA Boston.
Marcus Ruopp, MD
Email: Marcus.Ruopp@va.gov
ORCID ID: 0000-0002-4129-2762
Marcus Ruopp is the Associate Chief of Geriatrics and Extended Care and the Medical Director for a Skilled Nursing Facility (Community Living Center) at the VA Boston Healthcare System. After completing training in Internal Medicine at Duke University Medical Center, he joined the faculty at VA Boston Healthcare System and Harvard Medical School. He completed a Rabkin Fellowship in Medical Education at the Shapiro Institute for Education and Research at Harvard Medical School and Beth Israel Deaconess Medical Center and the Society of General Internal Medicine (SGIM) TEACH certificate program. His innovation and research are directed at improving post-acute care for older adults.
References
American Association of Nurse Practitioners. (2023, November). NP fact sheet. American Association of Nurse Practitioners.
Bryant, S., & Parker, K. (2019). Participation in a nurse practitioner fellowship to instill greater confidence, job satisfaction, and increased job retention. Journal of the American Association of Nurse Practitioners, 32(10), 1. https://doi.org/10.1097/jxx.0000000000000313
Caplan, Z., & Rabe, M. (2023, May). The older population: 2020. 2020 census briefs. https://www2.census.gov/library/publications/decennial/2020/census-briefs/c2020br-07.pdf
Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine. (2011). The future of nursing: Leading change, advancing health. National Academies Press. https://nap.nationalacademies.org/read/12956/chapter/1#xi
Faraz, A. (2019). Facilitators and barriers to the novice nurse practitioner workforce transition in primary care. Journal of the American Association of Nurse Practitioners, 31(6), 364–370. https://doi.org/10.1097/jxx.0000000000000158
Meissen, H. (2019). Nurse practitioner residency and fellowship programs. Journal of the American Association of Nurse Practitioners, 31(7), 381–383. https://doi.org/10.1097/jxx.0000000000000255
Pleshkan, V., & Hussey, L. (2020). Nurse practitioners’ experiences with role transition: Supporting the learning curve through preceptorship. Nurse Education in Practice, 42, 102655. https://doi.org/10.1016/j.nepr.2019.102655
Span, P. (2020, January 3). Older people need geriatricians. Where will they come from? The New York Times. https://www.nytimes.com/2020/01/03/health/geriatricians-shortage.html
U.S. Department of Veterans Affairs. (2024). Geriatric and extended care nurse practitioner residency training program. https://www.va.gov/boston-health-care/work-with-us/internships-and-fellowships/nurse-practitioner-residency-programs/#geriatrics-and-extended-care-n
Vespa, J. (2018, March 13). The graying of America: More older adults than kids by 2035. The United States Census Bureau. https://www.census.gov/library/stories/2018/03/graying-america.html
