


Approaching the topic of Advance Care Planning (ACP) with patients and families is often difficult, overwhelming, uncomfortable, and, unfortunately, too late. Over the past 30 years, numerous organizations have been established to identify and find solutions that bridge the knowledge gap between healthcare professionals and patients, while honoring a patient’s values, goals, and wishes. This gap created the need for ACP. Strategies and tools to guide healthcare professionals and patients can facilitate less difficult, more effective, and timely conversations among patients, families, and providers. In this article, we present numerous strategies and tools used in ACP by examining a fictional case study exemplar about an individual who is fairly advanced along the continuum of advance care planning. The complexities of the case study further accentuate the need for strategies and tools in ACP conversations and discusses those that we have used in practice. Included also are supplemental materials that offer definitions, and outline strategies and tools that can be helpful for healthcare professionals, patients and families, or anyone interested in addressing ACP.
Key Words: Advance Care Planning (ACP), ACP tools, ACP strategies, shared decision-making, end-of-life decisions, POLST, goals of care, serious illness conversations, patient autonomy, choices
Approaching the topic of Advance Care Planning (ACP) with patients and families is often difficult, overwhelming, uncomfortable, and, unfortunately, too late. The Patient Self-Determination Act of 1990 ([PSDA], Congress.gov, H.R., 4449, 1989-1990) was a federal law which created a need for more information about healthcare and choices in the future for patients and families. Before this law, most healthcare decisions had been made by physicians. Over the past 30 years, numerous organizations have been established to identify and find solutions that bridge the knowledge gap between healthcare professionals and patients, while honoring a patient’s values, goals, and wishes. This gap created the need for Advance Care Planning (ACP). Advance care planning is much more than advance directives and can be complex.
Advance care planning is much more than advance directives and can be complex. However, the importance of timing and implementing strategies and tools for ACP are often key factors (Hooper et al., 2020; Sedini et al., 2022; Sudore et al., 2017) . Looking back to high school courses where financial planning for life is taught, including ACP for health conditions and potential life-limiting conditions in the coursework would be ideal (National Institutes for Health [NIH], 2022; shine365, 2018). However, ACP does not occur in these courses. If it did, ACP strategies and tools would help persons facing a healthcare crisis (e.g., a car accident or acute medical illness) to have choices about the care they receive.
In 2017, Izumi and Fromme (2017) addressed the importance of decision-making at different stages of a person’s life with the needed conversations and documentation as an ACP continuum (See Figure). Numerous strategies and tools can be used, both by healthcare professionals and patients (aka, client, consumer) involved along this ACP continuum.
Figure. Continuum of Advance Care Planning
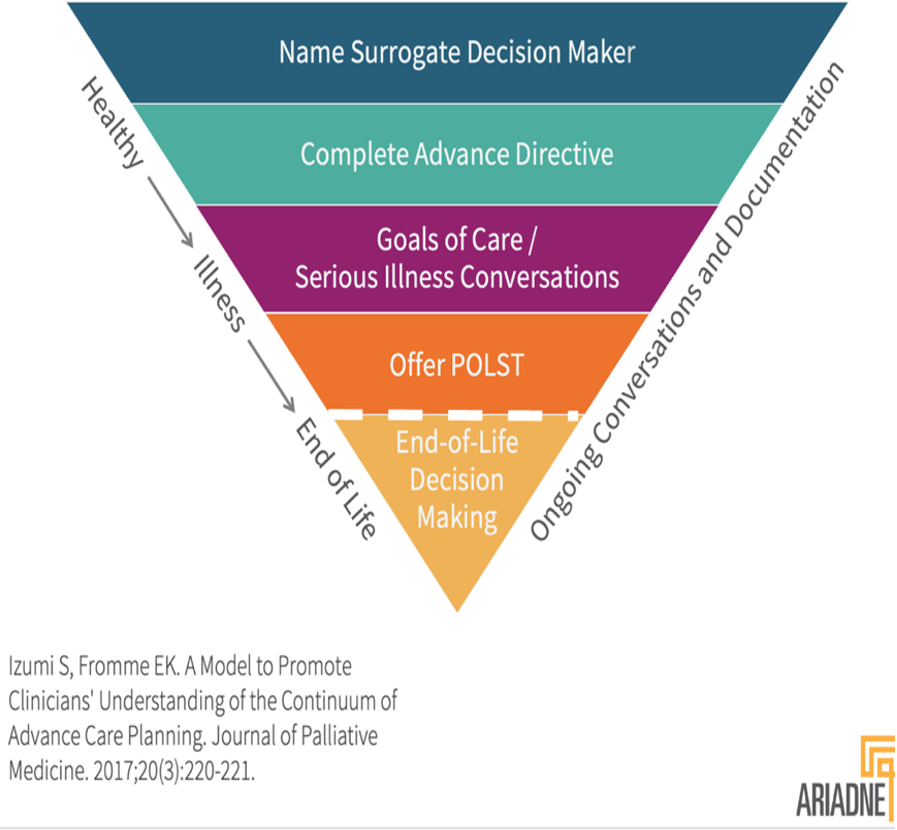
(©Reprinted with permission, granted 7.27.25)
When determining strategies and tools to use, factors to consider include the methods of communication (e.g., written, verbal, audiovisual) and who is present in the conversation (Winnifrith et al, 2024). How the patient may try to avoid the conversation also needs to be considered (Zwakman et al, 2021). It is more important to have patients express their wishes than to rely on family or friends for answer(s); however, a patient may not truly agree with the choices the family makes (Sudore, 2022). There are various strategies and tools to facilitate ACP discussions. This article will present examples of strategies and tools that can be useful to providers and patients for discussions across the ACP continuum. When determining strategies and tools to use, factors to consider include the methods of communication and who is present in the conversation
Different tools are used, based on the patient’s best method of learning in decision-making. These ACP tools include conversation guides, game-based video, web-based tools, patient portals, and decision aids that assist the healthcare professional in starting or continuing the conversations. The following three part case study exemplar will illustrate the different spectrums of Izumi and Fromme’s (2017) Continuum of Advance Care Planning model (see Figure), which includes ACP tools for healthcare providers and patients organized according to the health status of the patients. Many of these tools are further explained in the supplemental materials linked below.
Case Study Exemplar
Case Study Kenneth: Part I
“Kenneth” is a fictional patient created from a combination of several patients. Kenneth is a 65-year-old veteran with longstanding diabetes, hypertension, and chronic kidney disease who resides in Shady Oaks nursing home for care due to his additional diagnosis of dementia. The interdisciplinary care team of the nursing home work alongside his specialty care providers for nephrology, neurology, psychiatry, and palliative care. This extended team worked with Kenneth’s sister, Louise (his guardian), to develop goals of care for Kenneth, based on his verbalized wishes. Multiple conversations have occurred to discuss the team’s inability to obtain routine bloodwork due to Kenneth’s fear of needles. The seeds for advance care planning were sown early in the team's relationship with Louise and the interdisciplinary team members. In general, and in Kenneth’s case, advance care planning (ACP) is not a one-time conversation.
In general, and in Kenneth’s case, advance care planning (ACP) is not a one-time conversation. Like a seed, this planning is best sown early in the relationship between physicians, nurses, and other members of the healthcare team, and the individual patient, and the patient’s family or healthcare proxy. ACP is based on an understanding of the total person, including mind, body, soul, individualized wishes, belief system, and their very existence (Institute of Medicine [IOM], 2015). By applying the ACP Continuum model, this case study exemplar will address each spectrum of the model.
Spectrums 1 and 2: Naming the Surrogate Decision-Maker and Complete Advance Directive
The first spectrum, Naming the Surrogate Decision-Maker, was not completed in Kenneth’s case. Kenneth was not competent nor had the capacity to make his own decisions, but he liked and trusted his sister, Louise. Upon her agreement, she was appointed his guardian. In Kenneth’s case, the second spectrum, Complete Advance Directive, was also not completed. An advance directive is solely the voice of the patient. Kenneth was not always consistent with his wishes, and Louise was not legally able to complete one on his behalf. An advance directive is solely the voice of the patient.
Most healthcare providers have not had basic education regarding the spectrum Naming a Surrogate Decision-Maker (which is based on laws of the state for Completing an Advance Directive ). Healthcare providers need to seek continuing education and additional training for these two spectrums of the continuum to better serve patients. Some providers may ask other healthcare professionals (i.e., not nurses) to work with patients in these spectrums of the continuum.
The first and foremost strategy to improve advance care planning in the healthcare professional’s approach is patient-centered communication (Bernacki et al., 2014). This strategy is crucial for each member of the team. Empathy is a key component to honest and open conversations which assist patients and their families to understand serious illnesses and help them to make informed decisions, based on a patient's wishes. Seminal articles, such as Suchman et al. (1997), have addressed empathy as a technique to set the stage. Clear communication between the patient and family and the interdisciplinary team is paramount for the individual patient care plan. The first and foremost strategy to improve advance care planning in the healthcare professional’s approach is patient-centered communication.
The word LISTEN, when the letters are rearranged, teaches us that we need to be SILENT. We need to hear precisely what the patient is saying and meet them where they are. Most importantly, we need to learn the power of a pause. A pause is a moment to reflect, revise, rephrase, and redirect the conversation, is based on what the patient says and understands. Put simply: talk less and listen more.
In addition, healthcare professionals need to reflect on the patient’s understanding of the situation in which they find themselves, revise the current available information, rephrase the information in bite-sized bits that are easier for the patient to digest, and redirect the conversation, based on all the above. Allowing patients and families to know that they are in control and that the decision is theirs sets the stage for a better understanding from both sides about exactly what the next steps will be. We need to hear precisely what the patient is saying and meet them where they are.
Listening to exactly what patients are trying to communicate, regarding their goals for themselves, is a key strategy often overlooked by many healthcare teams today. Although healthcare professionals may believe they have listened to their patient closely, often when checking back with the patient, that understanding is not the case. The healthcare professional may find that the patient has not communicated all of their wishes. Patients may have had a more in-depth conversation with other interdisciplinary team members about the information provided at the time and how they were made to feel during these challenging conversations (Back et al., 2009; Joyner, 2024). Listening becomes crucial. Listening to exactly what patients are trying to communicate, regarding their goals for themselves, is a key strategy often overlooked...
Healthcare professionals must realize that the same patient, on the same day, may speak with a nurse and say one thing and then speak with clergy and communicate something completely different. Finally, in speaking with the physician or another healthcare team member, that patient tells a new version based on their comfort level with that individual. When the patient has developed a relationship and the team understands what the individual wishes and goals are, advance care planning becomes a natural stop instead of a forced decision (Bernacki & Block, 2014; Izumi & Fromme, 2017, Madni, 2024). With everyone in agreement, the patient’s individualized plan of care can be established. In addition to listening to patients, healthcare professionals need to be aware of the different spectrums of the ACP Continuum model and how different ACP strategies and tools can be used for this case and other situations. See Supplemental Materials A linked below for a detailed list of the strategies used throughout this case study exemplar with reference information and definitions and/or/brief summaries as applicable.
Most ACP tools include professional training through online learning and continuing education. The tools that we used for this case study exemplar included the following: a) Respecting Choices®, b) Honoring Choices (state specific) c) Hospice and Palliative Nurses Association (HPNA), d) The Center to Advance Palliative Care (CAPC), e) Education in Palliative and End-of-Life Care (EPEC), f) End of Life Nurses Education Consortium (ELNEC), g) Fast Facts, and h) The National Clinical Practice Guidelines for Quality Palliative Care. Refer to the Supplemental Materials B linked below for a more extensive list of ACP tools for healthcare providers. Most ACP tools include professional training through online learning and continuing education.
There are also ACP tools for patients. ACP tools for patients used by these authors included the following items: a) The Go Wish Card Game, b)The Conversation Project®, c) GetPalliativeCare.org, d) state-specific advance directives (aka healthcare directive, living will, durable power of attorney for healthcare), e) MyDirective.com, and f) portal-based advance care planning or advance directives. Please refer to the Supplemental Materials B linked below for more information about ACP tools for patients and families. There are also ACP tools for patients.
Case Study Kenneth: Part 2
As the case study continues, Kenneth’s condition changes. Nurses have noted increased behavioral outbursts while awake, more sleeping, a poor appetite, and low urine output. He appeared to have dyspnea and would be fatigued easily with his usual activities. The nurse notified the primary care team, who awaited an opportunity to arrange for laboratory testing; this was met with resistance by Kenneth. After a conversation with Louise, Kenneth finally agreed to have blood drawn. Kenneth was able to give a urine sample as well. Laboratory results revealed critically elevated potassium, blood urea nitrogen (BUN), and creatinine levels. He was also severely anemic, and his urine sample was concentrated with low pH and elevated glucose. Based on the findings, nephrology and psychiatry consultants for Kenneth were contacted. Keeping in line with his wishes, oral medications were initiated to lower his potassium levels, and his antipsychotic medications were titrated. Additional wishes included no hospitalizations, no intravenous (IV) fluids, and no blood transfusions; these wishes were honored.
The situation was complicated by his resistance to taking oral medications and the urgent need to reduce his potassium. Nephrology recommended urgent dialysis and insertion of a temporary dialysis catheter. An interdisciplinary team meeting was convened. Louise was upset and confused about what to do. When she was reminded of the earlier conversations regarding Kenneth’s refusal to allow blood draws and his fear of needles, she was able to understand that she would need help to navigate the available choices.
In retrospect, aspects of the Izumi and Fromme (2017) ACP Continuum model were helpful to the care team and Louise. The next section considers more specifically how this model was utilized to inform decisions about whether or not to pursue dialysis for Kenneth. Palliative care teams are known for their skills in advance care planning.
Utilizing the ACP Continuum Model
The ACP Continuum model (Izumi & Fromme, 2017) parallels a palliative care framework. Palliative care should be a part of any serious illness journey. The interdisciplinary team will provide symptom management, care coordination, psychological, and spiritual support as well as bereavement support to all involved family members. Palliative care teams are known for their skills in advance care planning.
Thinking in the context of our previous planting metaphor, cultivating the environment and preparing the ground allows the seed set earlier in the relationship to grow and flourish. This happens while watering it with nutrients, in this case, the palliative care ABCs: a) respect for individual autonomy, b) belief in the understanding of individual fears related to serious illness, and c) compassion for the emotions the patient and family are facing, having to make complex decisions, create the ideal foundation for continued conversation, and goal setting in the face of serious illness (Rosa et al., 2023).
When the conversation addressed advanced renal disease, the team continued to cultivate Kenneth’s environment by developing a relationship with Louise and understanding that Kenneth had clearly stated his wishes and emotions over time. Additionally, incorporating the team's observations regarding needles, routine blood draws, and Kenneth’s inability to sit for extended periods was beneficial. The conversations, related earlier in the illness, allowed for building a good foundation when the time came to discuss the inevitable dialysis.
The team was able to discuss goals of care, Kenneth's wishes, and identify concerns Louise had about whether to pursue dialysis. Ultimately, the team created a plan to have a dialysis simulation, which was discussed with the nephrologist, the psychiatrist, the nursing home team, the palliative care physician, and risk management. Using simulation was an unconventional way to help Kenneth and Louise ultimately conclude the next steps in his individualized care plan regarding his serious illness. Kenneth did not tolerate the dialysis mock session due to the time commitment required for him to sit still, the repeated number of blood draws required to manage his care, and his individual vocalized wish not to have to pursue this avenue of care for him. Ultimately, the team created a plan to have a dialysis simulation...
This mock experience helped identify the choices for Louise, who now had additional insight into what her brother wanted for himself, how he chose to live, and ultimately how he chose to die. This discernment led to frequent conversations about his wishes and what he wanted to achieve in his remaining time of life. This understanding contributed to a comprehensive plan of care regarding Kenneth's wishes, wants, and goals, and solidified decisions in advance that ultimately assisted Louise through the entire shared decision-making process about his clinical care. Strategies, such as those mentioned above, assist family members in a time when shared decision-making is complex, and many emotions often lead to misguided decisions.
Spectrum 3: Goals of Care/Serious Illness Conversation
In the next spectrum, During Serious Illness Conversations, many palliative care providers have been trained in EPEC or ELNEC for advance care planning conversations and identifying patients appropriate for those conversations (See appendix A). Other healthcare providers may have had training through the Respecting Choices® program in their health systems. Baxter et.al. (2022) describes how the surprise question, “Would you be surprised if the patient died in the next six months”, is used for identification of potential hospice patients. However, this question was modified to say, “would you be surprised if the patient died in the next one to two years” which allows for earlier, facilitated discussions using the Serious Illness Conversation Program and Guide (Ariadne Labs 2023, Ariadne Labs 2024, Ariadne Labs 2025).
In spectrum 3, we used the following ACP tools for this case: a) the Serious Illness Care Program, the b) Serious Illness Conversation Guide, c) Vital Talk d) Vital Talk Tips app (both Apple and Google Play) e) C-TAC (Coalition to Transform Advanced Care) and f) Fast Facts (PCNOW, 2025). Supplement A provides additional guidance for healthcare professionals. The ACP tools we recommended for patients to use included: a) GetPalliativeCare.org, b) Hard Choices for Loving People (Dunn, 2016) and c) Go Wish Cards (Coda Alliance, 2025) (see Supplemental Materials C). We also used simulations and virtual reality videos which is beneficial for patients, families and healthcare providers alike (Parekh de Campos, & Polifroni, 2023). When utilizing simulation, the team should include palliative care team, clergy, psychology, nursing, and child life specialist (if indicated) as well as specialists for the different procedures (Hsieh, 2020). These types of tools are very beneficial for healthcare providers to portray actual scenarios and for patients and families who are making healthcare decisions. More time may be required to set a simulation up, but the outcome is clear with the choice the patient makes, as is also evident in our case study exemplar scenario (Ellis, 2019; Irvine & Spence, 2025; Parekh de Campos & Polifroni, 2023; Pereira-Salgado et al, 2019). The table offers additional examples of possible ACP simulations.
Table. Possible ACP Simulation Examples
|
ACP Simulation Examples |
Specialists (plus others*) |
|---|---|
|
CPR |
EMS |
|
Dialysis |
Nephrology |
|
Intubation / ventilation |
EMS/ICU / Pulmonary |
|
Enteral nutrition / Medical hydration and nutrition |
GI/ Interventional Radiology / Special Procedures / Dietitians / Speech |
|
Implantable Cardioverter-Defibrillator (ICD) |
Cardiology |
|
Extracorporeal Membrane Oxygenation (ECMO) |
Cardiology / Pulmonary |
|
Left Ventricular Assist Devise (LVAD) |
Cardiology |
* Include palliative care team, clergy, psychology, nursing, and child life specialist (when indicated) for the different procedures (Hsieh, 2020).
Following the serious illness conversations on the spectrum, we proceed to Physician Orders for Life-Sustaining Treatment , or POLST (National POLST, 2018).
Spectrum 4: Offer POLST
Spectrum 4, Offer POLST (i.e., Physician Orders for Life-Sustaining Treatment), refers to a nationally known portable medical order and a part of ACP when a person is facing serious illness. This concept may be under different names in each state and. A POLST medical order form accompanies the patient and is used in conjunction with the advance directive (Joyner et al., 2019; National POLST, 2022). Both authors have had training in POLST through the National POLST organization. Other healthcare professionals may use statewide education or national education for POLST (refer to Supplemental Materials B).
The ACP tools about POLST that we recommend for patients include: a) POLST: Portable Medical Orders and b) POLST form (refer to Supplemental Materials C) The Serious Illness Conversation and the POLST medical order form were used in Kenneth’s fictional case.
Case Study Kenneth: Part 3 and Spectrum 5: End-of-Life Decision Making
The key feature in Kenneth's case study exemplar was utilizing seeds that were sown much earlier in the team's relationship with him and his sister, Louise. Strategies included value-based care, where Kenneth’s treatment was aligned with what mattered most to him: his comfort, wishes, and symptom relief. Nurturing those seeds and watering them with the knowledge of the interdisciplinary team’s abilities to approach Kenneth's care led to deeper conversations. Based on his verbalized wishes, once those seeds had sprouted and the situation arose where Louise was respecting Kenneth’s wishes, she had to make a difficult choice. However, Louise and Kenneth felt supported, nurtured, and knowledgeable because of the open conversations that had taken place. The key feature in Kenneth's case study exemplar was utilizing seeds that were sown much earlier in the team's relationship with him and his sister, Louise.
Louise and Kenneth saw transparency in action as each of the team members continuously communicated with them and among each other. Being able to focus on Kenneth's quality of life while supporting his clinical condition with mock dialysis, respected Kenneth's choices and supported Louise in making appropriate medical decisions. Kenneth was able to enjoy movies at the theater, eat popcorn, play Bingo, go on recreational outings, and participate within his ability without any restrictions to his diet or activities. This strategy created a seamless shift from disease management to patient-centered care and quality of life (IOM, 2015). (See Supplemental Materials A linked above for the list, definitions and references of the strategies used throughout this case study). Being able to focus on Kenneth's quality of life while supporting his clinical condition with mock dialysis, respected Kenneth's choices and supported Louise...
A patient tool often used near the end of life is the booklet, Gone from My Sight, by Barbara Karnes (1986), known by hospices nationally as the “little blue book.” This booklet was given to Louise, but surprisingly, Kenneth wanted one as well. The care team watched his reaction, but Kenneth paged through the booklet and then put the booklet in the garbage.
Conclusion
In summary, this case study reflects the use of strategies and tools that can be helpful to facilitate advance care planning. The discussion has also demonstrated the need for teamwork and communication among different healthcare professionals and family involved in the shared decision-making process. Utilizing a continuum of ACP guides, healthcare professionals, patients, and families alike can be informed as to what choices may be needed in the future. Strategies and tools presented in this article can assist the interdisciplinary team and the patient/family to inform shared decision-making and honor the patient’s goals, wishes, and values. Finally, cultivating the ABCs (i.e., autonomy, beliefs, and compassion) in Kenneth’s fictional case study, and in real practice, ensures the long-term sustainability of quality of life.
Authors
Nancy E. Joyner, MS, CNS-BC, APRN, ACHPN®
Email: njoyner@nancyjoyner.com
Nancy Joyner, MS, CNS-BC, APRN, ACHPN® has a BA degree from Bemidji State University, MN, in pre-medicine, biology, and both a BSN degree in Nursing and an MS degree in Nursing Therapeutics from the University of North Dakota, Grand Forks, ND. She is a certified Palliative Care Clinical Nurse Specialist with over 20 years of clinical and educational practice. Nancy is one of the trained Ariadne Lab facilitators for MN’s Center to Advance Serious Illness Conversation (CASIC), a program that provides healthcare professionals with strategies (including drills and virtual practice) to enhance Advance Care Planning (ACP) across all disciplines.
Kavita Sharma, MD, FAAHPM®
Email: mdoflb@gmail.com
Kavita Sharma, MD, FAAHPM® served in leadership roles at the Department of Veterans Affairs in Chicago and at Calvary Hospital Hospice and Home Care in the Bronx, New York. She has experience and certification in Internal Medicine, Geriatric Medicine, and Hospice & Palliative Care. Dr. Sharma specializes in Compensation & Pension evaluations and Military Environmental Health. As a Fellow of the American Academy of Hospice and Palliative Medicine, Dr. Sharma also serves as a Clinical Assistant Professor of Medicine at RFUMS. Her clinical practice is deeply patient-centered, guided by the individual goals and wishes of her patients. Dr. Sharma focuses on helping patients live well with serious illnesses and preserving their quality of life through end-of-life care. She is a passionate advocate for holistic well-being and longevity, believing in healing that integrates the mind, body, and soul.
References
AACN. (2025). End-of-life nursing education consortium (ELNEC): Fact sheet. https://www.aacnnursing.org/Portals/0/PDFs/ELNEC/ELNEC-Fact-Sheet.pdf
Apple Inc. (2025). Vital talk tips app https://apps.apple.com/us/app/vitaltalk-tips/id1109433922
Ariadne Labs. (2025). Every person with serious illness is known and cared for on their own terms. https://www.ariadnelabs.org/serious-illness-care/
Ariadne Labs. (May 2023). Serious illness conversation guide. https://www.ariadnelabs.org/wp-content/uploads/2023/05/Serious-Illness-Conversation-Guide.2023-05-18.pdf
Ariadne Labs. (2024). The playbook: Better care for people with complex needs: The serious illness conversation guide. https://bettercareplaybook.org/resources/serious-illness-conversation-guide-0#:~:text=This%20tool%20offers%20care%20providers,prognosis%2C%20goals%2C%20and%20values.
Back, A. L., Bauer-Wu, S. M., Rushton, C. H.. & Halifax, J. (2009). Compassionate silence in the patient-clinician encounter: a contemplative approach. Journal of Palliative Medicine, 12(12), 1113-7. https://doi.org/10.1089/jpm.2009.0175. PMID: 19698026; PMCID: PMC2939848.
Baxter, R., Fromme, E. K., & Sandgren, A. (2022). Patient identification for serious illnessconversations: A scoping review. Int J Environ Res Public Health, 19(7), 4162. https://doi.org/10.3390/ijerph19074162
Bernacki, R. E., & Block, S. D. (2014). Communication about serious illness care goals: A review and synthesis of best practices. JAMA Intern. Med., 174,1994–2003. https://doi.org/10.1001/jamainternmed.2014.5271
Center to Advance Palliative Care (CAPC). (February 3, 2025). Clinical tools for deliveringhigh quality care. https://www.capc.org/toolkits/clinical-tools-delivering-high-quality-care/
Coda Alliance. (2025). Take responsibility, choose your own way, embrace life. https://codaalliance.org/
Congress.gov. (1989-1990). H. R. 4449-Patient Determination Act of 1990. 101st Congress. Available: https://www.congress.gov/bill/101st-congress/house-bill/4449
Conversation Project, The. (2025). About us. https://theconversationproject.org/
Dunn, H. (2016). Hard choices for loving people (6th ed). https://hankdunn.com/product/hard-choices-for-loving-people/
Ellis, B., Winn, S., MacMillan, D., & Bouithillet, K. (Dec 19, 2019). A simulated learningexperience in advanced care planning conversations. https://kb.gcsu.edu/cgi/viewcontent.cgi?params=/context/dnp/article/1035/&path_info=auto_convert.pdf
Hsieh, W,T. (2020). Virtual reality video promotes effectiveness in advance care planning. BMC Palliat Care 19:12. https://doi.org/10.1186/s12904-020-00634-w
Hooper, S., Sabatino, C. P., & Sudore, R. L. (2020). Improving medical-legal advance careplanning. Journal of Pain and Symptom Management, 60(2), 487-494. https://doi.org/10.1016/j.jpainsymman.2020.03.004
Hospice & Palliative Nurses Association. (HPNA). (2025). Advanced care planning. https://www.advancingexpertcare.org/practice-research/resource-pages/advance-care-planning/
Institute of Medicine (IOM). (2015). Dying in America: Improving quality and honoring individual preferences near the end of life. National Academies Press.
Irvine, J., & Spence, A. (2025). What is known about simulating advance care planningdiscussions for healthcare professionals and its impact on patients and learners? Future Healthcare Journal, 12(2) Supp100446, 2514-6645. https://doi.org/10.1016/j.fhj.2025.100446
Izumi, S., & Fromme, E. K, (2017). A model to promote clinicians' understanding of thecontinuum of advanced care planning. Journal of Palliative Medicine, 20(3), 220-221. https://doi.org/10.1089/jpm.2016.0516
Joyner, N., Palmer, C., & Hatchett, J. (October 15, 2019). The pearls of physician orders for life sustaining treatment (POLST): Translating patient decisions into treatment orders. OJIN: The Online Journal of Issues in Nursing, 25(1). https://doi.org/10.3912/OJIN.Vol25No01PPT47
Joyner, N. (March 26, 2024). The four Cs of palliative care: Comfort, communication, choices & control: Basics for providers & healthcare professionals/clinicians. https://www.amazon.com/Four-Palliative-Care-Communication-Professionals/dp/099885851X#:~:text=Nancy%20Joyner-,The%20Four%20Cs%20of%20Palliative%20Care:Comfort%2C%20Communication%2C%20Choices,for%20Providers%20&%20Healthcare%20Professionals/Clinicians
Karnes, B. (1986). Gone from my sight: The dying experience. https://bkbooks.com/products/gone-from-my-sight-the-dying-experience
Lum, H. D., Brungardt, A., Jordan, S. R., Phimphasone-Brady, P., Schilling, L., Lin, C., & Kutner, J. (2019). Design and implementation of patient portal–based advance care planning tools. Journal of Pain and Symptom Management, 57(1), 112-117.e2. https://pubmed.ncbi.nlm.nih.gov/30595147/
Madni, A. (May 28,2024). Culturally responsive care for patients with a serious illness. #478. Journal Pall Med 27 (5):699-701. https://doi.org/10.1089/jpm.2024.0059
MyDirectives. (2025). Make your wishes known. https://www.mydirectives.com/
National Consensus Project for Quality Palliative Care. (2018). Clinical practice guidelinesfor quality palliative care (4th edition). https://www.nationalcoalitionhpc.org/ncp-guidelines/
National POLST. (2018). Founders story celebrating a unique grassroots effort that grewinto a national movement. https://polst.org/wp-content/uploads/2022/02/2018.12.04-POLST-Founders-Story.pdf
National Institute of Health (NIH): National Institute on Aging. (October 31, 2022). Advanced care planning: Advance directives for healthcare. https://www.nia.nih.gov/health/advance-care-planning/advance-care-planning-advance-directives-health-care#:~:text=Download%20the%20PDF-,What%20are%20advance%20directives?,choosing%20a%20health%20care%20proxy
Northwestern Medicine. (2025). EPEC: Education in palliative and end-of-life care. Available: https://www.bioethics.northwestern.edu/programs/epec/index.html
Palliative Care Network of Wisconsin (PCNOW). (2025). Fast facts.https://www.mypcnow.org/fast-facts/
Parekh de Campos, A. & Polifroni, C. E. (2023). Development of a standardized simulation: Advance care planning conversations for nurses. Nursing Research. https://doi.org/10.1097/NNR.0000000000000625 https://www.aacnnursing.org/Portals/0/PDFs/ELNEC/Advance-Care-Planning-Conversation-CHATT-Conversations-Had-at-Trying-Times-Simulation.pdf
Pereira-Salgado, A., Philpot, S., Schlieff, J., Driscoll, L. & Mills, A. (2019). Advance careplanning simulation-based learning for nurses: Mixed methods pilot study. Clinical Simulation in Nursing, 29, 1-8. https://www.nursingsimulation.org/article/S1876-1399(18)30124-5/pdf#:~:text=Simulation%2Dbased%20learning%20(SBL)%20enables%20education%20de%2D,ducting
Respecting Choices. (n.d.). About us. Available: https://respectingchoices.org/about-us/
Rosa, W. E., Izumi, S., Sullivan, D. R., Lakin, J., Rosenberg, A. R., Creutzfeldt, C. J.,Lafond, D., Tjia, J., Cotter, V., Wallace, C., Sloan, D. E., Cruz-Oliver, D. M., DeSanto-Madeya, S., Bernacki, R., Leblanc, T., & Epstein, A.S. (2023). Advance care planning in serious illness: A narrative review. Journal of Pain Symptom Management, 65(1), e63-e78. https://pubmed.ncbi.nlm.nih.gov/36028176/
Sedini, C., Biotto, M., Crespi Bel'skij, L. M., Moroni Grandini, R. E., & Cesari, M. (2022). Advance care planning and advance directives: An overview of the main critical issues. Aging Clin Exp Res. 34(2), 325-330. https://doi.org/10.1007/s40520-021-02001-y
shine365. (April 16, 2018). Why high school seniors need an advance directive. https://shine365.marshfieldclinic.org/wellness/advance-directives-teenagers/#:~:text=Advance%20care%20planning%20is%20about,Complete%20an%20advance%20directive
Suchman, A.L., Markakis, K., Beckman, H.B. & Frankel, R. (1997). A model of empathic communication in the medical interview. JAMA 277(8):678-82. PMID: 9039890. https://pubmed.ncbi.nlm.nih.gov/9039890/
Sudore, R. (May 6,2022). Advance care planning: What is it and when should it be done? Available: https://www.ncoa.org/article/advance-care-planning-what-is-it-and-when-should-it-be-done/
Sudore, R. L., Lum, H. D., You, J. J., Hanson, L. C., Meier, D. E., Pantilat, S. Z., Matlock, D. D.,Rietjens, J. A. C., Korfage, I. J., Ritchie, C. S., Kutner, J. S., Teno, J. M., Thomas, J., McMahan, R. D., & Heyland, D. K. (2017). Defining advance care planning for adults: A consensus definition from a multidisciplinary Delphi panel. J Pain Symptom Manage, 53(5):821-832.e1. https://doi.org/10.1016/j.jpainsymman.2016.12.331
Winnifrith, T., Millington-Sanders, C., Husbands, E., Haros, J., & Ballinger, H. (2024). Proactive advance care planning conversations in general practice: a quality improvement project. BMJ Open Qual.13(3), e002679. https://doi.org/10.1136/bmjoq-2023-002679. PMID: 38977313; PMCID: PMC11256018.
Zwakman, M., Milota, M. M., van der Heide, A., Jabbarian, L. J., Korfage, I. J., Rietjens, J. A.C., van Delden, J. J. M., & Kars, M. C. (2021). Unraveling patients' readiness in advance care planning conversations: A qualitative study as part of the ACTION Study. Support Care Cancer, 29(6), 2917-2929. https://doi.org/10.1007/s00520-020-05799-x. https://pmc.ncbi.nlm.nih.gov/articles/PMC8062377/#:~:text=of%20being%20ready.-Signs%20of%20not%20being%20ready,deterioration%20of%20health%20or%20death
