


Advance care planning (ACP) is a shared decision-making process that promotes self-reflection, discussion, and documentation of future healthcare preferences for clients, families, and clinicians, including nurses. However, members of the lowest socioeconomic status (SES) communities are 33% less likely to use ACP compared to those with the highest SES, which is why our research has focused on understanding barriers and facilitators to ACP for these low SES populations. In this article, we have summarized and synthesized barriers and facilitators to ACP across four publications that have reported our previous qualitative studies. We discuss five emerging themes from this synthesis: 1. Healthcare, Health Insurance, and Health, 2. Structural Factors, 3. Interpersonal Factors, 4. Religious Beliefs, and 5. Personal Factors. Our discussion considers the five themes in the context of the nurses’ role to provide ACP for clients with the lowest socioeconomic status. These considerations include understanding the roots of historical mistrust in healthcare institutions, and connections between nurses and clients to initiate ACP topics while validating reasons for healthcare mistrust. Nurses can also use a holistic approach to address structural barriers to ACP by using their inherent skills to assess social needs and make interdisciplinary referrals. Finally, we discuss considerations for integrating families into ACP conversations, addressing religious beliefs for or against ACP, and using trauma-informed approaches.
Key Words: advance care planning, nursing, socioeconomic status, income, qualitative research, palliative care, barriers, facilitators, living will, advance directive
Advance care planning (ACP) is often underused and misunderstood. Yet this beneficial communication process supports preparation for future care that people may receive during healthcare emergencies and, in some cases, a shift from acute to supportive care (Hickman et al., 2023; McMahan et al., 2024; Sudore et al., 2017). The ACP process is defined as an ongoing communication process designed to enable learning about key ACP concepts, prepare clients and families for healthcare decision-making during a crisis, and discuss and document the client’s preferences and values (Sudore et al., 2017). An updated definition of ACP includes a spectrum of care planning for present, future, and end-of-life treatments and therapies. Clients and families weigh the benefits versus the burden of treatment options and consider what option(s) will promote their uniquely defined quality of life (Hickman et al., 2023). An updated definition of ACP includes a spectrum of care planning for present, future, and end-of-life treatments and therapies.
Overall, ACP participation has increased, but sizable gaps persist between members of the lowest and the highest socioeconomic status (SES) communities (Barwise et al., 2019; Inoue, 2016; Nouri et al., 2020). In the past five years, we have employed qualitative research methods to investigate barriers and facilitators to ACP among low SES communities, particularly those in subsidized housing, thereby enabling a deeper understanding of why the problem exists, community priorities, and potential solutions. In this article, we will provide a summary of our findings, compare them with the ACP literature at large, and discuss implications for nursing practice in the final section. Overall, ACP participation has increased, but sizable gaps persist between members of the lowest and the highest SES communities.
Methods
Sample and Setting
We reviewed findings from four publications. All of the qualitative studies reported used thematic or content analysis of semi-structured interviews conducted in Nashville, TN between 2019 and 2022 (Coogan et al., 2022; Kimpel et al., 2022, 2024, 2025).
Data Collection and Analysis
In our studies, we interviewed housing specialists and older adults with low income. We used a modified matrix analysis approach to categorize and visualize the findings from each study (Averill, 2002). Key themes and subthemes were listed in two ...we interviewed housing specialists and older adults with low income.columns of a spreadsheet divided by barriers and facilitators, with each section of rows corresponding to an article (see Table). Using color coding to categorize findings into five themes, individual findings for each category were summarized. One challenge that arose during our synthesis is that the findings from each study were not initially framed as barriers and facilitators. To overcome this challenge, the matrix approach allowed us to visually compare factors that served as both barriers and facilitators (e and).g., religious beliefs, thus creating a more nuanced understanding and description of the phenomenon.
Table. Organization of Publication Findings for Synthesis
|
Abbreviated title, First author (first cell below the title) |
Facilitators |
Barriers |
|---|---|---|
|
Affordable housing specialists |
Housing workers as potential interventionists |
Daily life of physical health problems |
|
Housing as a Safe Haven |
Lack of socialization |
|
|
|
|
Insufficient material and financial resources |
|
|
|
Planning as a luxury |
|
Perspectives on aging and end of life |
Aging |
Other priorities (rent, food, nutrition for health) |
|
Injury or hospitalization |
Superstition or magical thinking |
|
|
|
Strong preferences to avoid suffering or die in peace |
Heavy topic |
|
|
Desire to prepare for EOL financials for family |
Stressful thinking far ahead |
|
|
Previous family discussions |
Lack of trust in healthcare system |
|
|
Belief to avoid LSM to be able to go heaven |
Lack of trust in clinician to honor their wishes |
|
|
Trusted family members |
Fear of not recovering if in the hospital |
|
|
|
Belief that God is in control |
|
|
|
Belief that doing ACP is not trusting in God's plan |
|
|
|
Lack of social support/no one to trust |
|
Life-stage and contextual factors |
Primary care clinician asking about a living will |
No primary care clinician |
|
Wanting to financially prepare family (life insurance) |
Competing healthcare costs or lack of insurance |
|
|
|
Preferences to avoid personal suffering based on death-related experiences |
Structural barriers and priorities (financial and material insecurity, transportation, housing) |
|
|
Preferences to prevent familial suffering based on death-related experiences |
Gaps in health insurance during adulthood |
|
|
Early planning in family |
Lack of planning in family |
|
|
Aging |
Avoidant or lack of trusted family members |
|
|
Receptive and trusted family members |
“Here and now” resilient coping |
|
|
Creative problem-solving coping |
Avoidant optimism or desire to avoid stress |
|
|
Religious belief in free will/duty to plan |
View that they were not sick or old enough |
|
|
Seeking family or health clinician support to plan |
Belief that God is in control |
|
Essential ACP intervention features |
|
|
|
Advocacy and reliability of service provider facilitating ACP |
Avoidant or reluctant individuals due to fear, apathy, or lack of understanding |
|
|
|
Person-centered care (listening, asking about priorities, providing support for learning difficulties) |
|
|
|
Onsite health or ACP services |
|
|
|
Prioritizing life insurance |
|
ACP=Advance care planning, LSM=Life-sustaining measures
Color coding: Health or healthcare-related; Structural; Intrapersonal; Religious; Personal
Findings
Housing Specialists and Participant Characteristics
Across three studies that we reported in four publications, key informants were housing specialists and older adults with low income. For this synthesis, housing specialists are referred to as housing specialists, and older adults with low income are referred to as participants. Overall, middle-age and older adults were aged 40+; primarily identified as Black or African American; had incomes <$20,000/year; and lived in subsidized housing. Housing costs were partially covered by public funds to reduce rent to ≤30% of the residents’ income (Alvarez & Steffen, 2021). Several participants across studies identified as Christian, or fairly or very spiritual or religious.
Emerging Themes
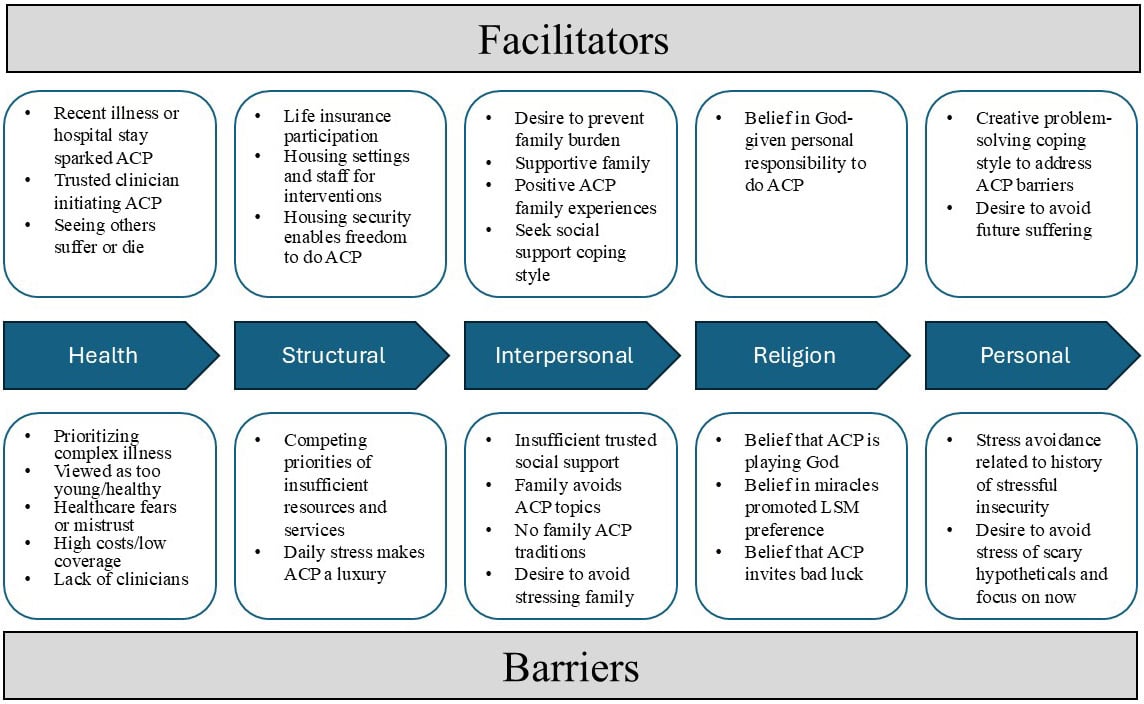
Five themes were identified in this synthesis: 1. Healthcare, Health Insurance, and Health, 2. Structural Factors, 3. Interpersonal Factors, 4. Religious Beliefs, and 5. Personal Factors. The Figure illustrates a summary of the facilitators and barriers associated with each theme. The following section further discusses these facilitators and barriers in greater detail, organized by theme.
Figure
Theme #1: Healthcare, Health Insurance, and Health
Health-related facilitators, including recent injuries, hospitalizations, or the aging process, represented circumstances that prompted conscious consideration of need, and underscored the urgency and relevance of ACP. Participants emphasized the importance of having a trusted primary care clinician to initiate ACP, such as offering an advance directive or a living will. We also found that participants’ previous experiences of seeing someone suffer in the healthcare setting or seeing someone die ...participants’ previous experiences of seeing someone suffer in the healthcare setting or seeing someone die informed their own preferences...informed their own preferences for life-sustaining measures. Such experiences prompted their interest in ACP and the desire to die in peace. Participants noted that effective ACP interventions should be included as part of on-site health services in subsidized housing settings with a person-centered care approach. This approach should consistant of actively listening to participants’ health priorities and providing learning aids for any comprehension barriers.
Housing specialists discussed how residents with low income often had experienced an earlier onset of poor physical health in life, and participants prioritized their chronic health concerns, such as affordable, proper nutrition for diabetes, over future care planning. Those with skepticism about ACP attributed their avoidance of planning to not being ill or old enough. Additional health-related barriers included healthcare avoidance due to fear that they would not be able to survive a hospital stay at their age, mistrust of a broken healthcare system, or lack of trust that clinicians would honor their wishes. Additional healthcare barriers that led to ACP avoidance were a lack of primary care clinicians, competing healthcare out-of-pocket costs, and gaps in health insurance during adulthood versus childhood or older adulthood when federal or state programs provided coverage. Those with skepticism about ACP attributed their avoidance of planning to not being ill or old enough.
Theme #2: Structural Factors
Facilitators included participants who had life insurance policies because they did not want their deaths to be a financial burden for family members. Additionally, housing specialists noted that subsidized housing provided a secure environment, or “safe haven,” to those with a history of being unhoused, making ACP a more viable option once housed. Additional implementation facilitators included subsidized housing as a community setting for ACP interventions and incorporating housing specialists as potential ACP initiators or interventionists. Notably, participants described that effective ACP interventionists should be reliable and advocate for their clients' holistic needs. An example of this was using closed-loop communication (i.e., following up with a client to confirm when a request has been completed). Additionally, an effective interventionist should provide warm handoffs for any referrals (e.g., providing a referral with a summary of the client’s background, needs, and what should be addressed). Housing specialists relayed that daily life was a struggle for residents...
Housing specialists relayed that daily life was a struggle for residents without sufficient transportation, food, nutrition, and other essential financial and material resources. These concerns and priorities were echoed by participants who communicated that everyday life was consumed by trying to address various forms of insecurity (e.g., food, transportation, medical needs). Structural barriers such as transportation and housing challenges preempted a sense of security necessary to support future-oriented thinking. In this way, housing specialists noted that competing structural priorities made ACP a seeming luxury that residents could not afford.
Theme #3: Interpersonal Factors
Family, when present and supportive, served as a facilitator for ACP. Prior family discussions with trusted family members who were receptive to such talks taught participants that they could rely on family members to have difficult conversations. On a personal level, the desire to prevent family suffering served as a motivator for planning. Participants who coped by seeking help from social ties were able to more easily envision using ACP with family members. Finally, witnessing previous generations, such as grandparents and parents, plan for aging and the end of life facilitated effective planning. ...the desire to prevent family suffering served as a motivator for planning.
Across the studies, participants discussed social and familial barriers. Housing specialists noted the lack of socialization due to estrangement from family. Some participants who lived in subsidized housing confirmed that they had no family or friends. If they did have social ties, some participants did not trust members of their social network to discuss their preferences should they become cognitively incapacitated or that their family would honor their preferences. Specifically, some participants with low-income spoke of family members who avoided discussing end-of-life topics, even when the participant was ready to do so. Another barrier was that planning was not a family tradition. Some participants also avoided ACP discussions with family because they did not want to worry or burden them with such stress. Participants identified a history of causing their family distress when they used illicit substances or alcohol, were incarcerated, or were unhoused, and did not want to add any ACP-specific stress on top of their past percieved indiscretions. Some participants who lived in subsidized housing confirmed that they had no family or friends.
Theme #4: Religious Beliefs
Religious beliefs served as a facilitator and a barrier for participants. For participants who perceived God as giving them a duty or the free will to engage in ACP, they reported a belief in personal responsibility to do ACP to fulfill their obligations. Other participants who viewed ACP as playing God, messing with God’s plan, or not trusting in God’s plan for their lives communicated hesitancy in engaging with ACP. Belief in miracles influenced Religious beliefs served as a facilitator and a barrier for participants.preferences, such as a desire to sustain life with life support in case a miracle occurs in the future. Some participants were hesitant to plan, because they viewed talking about the end of life as an invitation for bad things to happen.
Theme #5: Personal Factors
Participants who used creative problem-solving strategies to overcome barriers to planning were strongly motivated to use ACP and address challenges. Conversely, personal barriers included stress avoidance, which emerged out of comparing ACP with other stressful experiences, such as a history of socioeconomic insecurity, and wanting to avoid any unnecessary stress in thinking about ACP. Participants identified a priority to focus on present stressors and concerns that seem more concrete and real, rather than worrying about future hypothetical situations.
Discussion: Roles of Nurses
The purpose of this article was to summarize and synthesize our findings and provide nursing practice implications. In this section, we further consider the unique role of nurses to address the five categories of barriers and facilitators discussed above.
Addressing Healthcare Concerns
Our finding was that recent health events, such as hospitalizations, acted as an ACP facilitator. These acute events or diagnoses provide clinicians and nurses with an opportunity to frame the ACP discussion around an illness; ...recent health events, such as hospitalizations, acted as an ACP facilitator.however, nurses have identified insufficient time and training as significant barriers to initiating ACP with clients (Blackwood et al., 2019). Specifically, nurses report a lack of knowledge about legal policies and their scope of practice for ACP. This finding underscores the need for institutions and healthcare systems to promote ACP through financial support and protected time to learn about the legal and ethical regulations of ACP for nurses (Blackwood et al., 2019). For example, Medicare pays primary care nurse clinicians and clinical nurse specialists for 30 minutes of ACP during annual wellness visits (Services, 2025). Raising awareness among nurses is of the utmost importance to increase allowable billing by nurse clinicians related to ACP and enhance their confidence in fulfilling documentation requirements: the voluntary nature of the visit, advance directive education, an account of who attended the visit, and the visit duration (Services, 2025).
We also highlighted that illness and death-related experiences were importantfacilitators of ACP. The literature suggests that previous experience of others’ end-of-life experiences is associated with greater readiness for ACP in comparison to personal experiences of serious illness or surgery (Amjad et al., 2014). Nurses can facilitate clients’ exploration of their experiences of seeing loved ones receive medical care, express their ACP wishes, or make decisions for someone who was dying to identify personal values. However, experiences alone may not support ACP readiness. ...previous experience of others’ end-of-life experiences is associated with greater readiness for ACP...
We also found that mistrust of the healthcare system was a factor in ACP, but healthcare mistrust is a complex barrier in the literature that may vary by cultural and individual beliefs and experiences. For example, some literature has found that medical mistrust among Black or African American communities with low SES was a more substantial barrier to ACP compared to White Americans (Ward & Montgomery, 2024). While such findings may be true at the population level, clinicians should offer ACP as part of perso-centered care that promotes trust and power-sharing. These stereotyped assumptions promote avoidance and silence rather than embracing open and honest communication that reduces such inequities (Ashana et al., 2022). Nurses should practice cultural competency, exercise curiosity, and present the opportunity to engage in ACP with every client when able.
Addressing Structural Concerns
Throughout our studies, we have found that our participants from low SES communities face multiple layers of structural insecurity, leading to a cycle of uncertainty and stress. For example, healthcare insecurity encompasses questions about having sufficient insurance coverage, whether insurance will cover necessary expenses, the uncertainty of continued insurance, and what clients need to do to maintain coverage without feeling ashamed of their actions (e.g., breaking laws to afford out-of-pocket costs) (Whittle et al., 2020). It is vital for nurses to view clinical interactions as an opportunity to engage clients in ACP in a judgment-free space, abandoning preconceived notions that a client may not be interested because their problems seem insurmountable. A clinical interaction is a rare opportunity to build rapport and provide access to ACP education, which they may have previously avoided due to fear of financial burden or the risk of worsening their condition by seeking hospital care. ...our participants from low SES communities face multiple layers of structural insecurity, leading to a cycle of uncertainty and stress.
In addition to healthcare, financial, food, and housing insecurity, clients may face additional burdens (Whittle et al., 2020). For example, the burden of insecurity is often experienced as a unique stressor and stigma, defined as a social stain of dishonor related to a particular situation, characteristic, or individual (Oxford English Dictionary, n.d.). For clients with low SES, stigma may manifest in the shame of a diagnosis, fear of the social perception of not having a house or being lazy, and there is also the stigma of discussing death or life-limiting illness when thinking about ACP. Nurses are trusted professionals who can screen for social determinants of health with care and compassion, create care plans tailored to specific social needs, and identify and refer clients to community resources and services (National Academies, 2021). However, nurses alone do not have the time or capacity to address complex and multifaceted insecurity, and more dynamic and sustainable interventions are needed. For clients with low SES, stigma may manifest in the shame of a diagnosis, fear of social perception of not having a house or being lazy...
Several researchers have trialed community-level programs to integrate nursing with cross-disciplinary collaborations to address the complex barriers faced by clients with low SES. For instance, the Camden Core Model, originating in New Jersey, is a care management program intervention that employs a team-based approach, using nurses, social workers, and community health workers to provide hands-on coaching and care navigation (National Academies, 2021). Team members provide services such as medication reconciliation, care and service referrals, and escorting clients to their primary care appointments. This model, consistent with the caring philosophy of nursing, emphasizes a holistic, person-centric approach to clients through a genuine therapeutic connection.
While the New Jersey randomized controlled trials did not lead to reductions in hospital readmissions, similar programs in Philadelphia and Chicago have resulted in statistically and clinically significant reductions in hospital stays, urgent care visits, and healthcare costs (National Academies, 2021). For ACP, these care models offer a viable, nurse-led approach that may lead to long-term benefits, including improved outcomes for clients during health crises, reduced caregiver and family distress, and increased use of palliative and hospice care. Similar models are warranted to enhance relational nursing in communities, thereby building a solid foundation for difficult discussions and linking community settings to healthcare outcomes. One potential structural facilitator is integrating community health nursing within subsidized housing settings.
One potential structural facilitator is integrating community health nursing within subsidized housing settings. Pajka et al. (2023) explored perceptions of housing staff and residents regarding the implementation of an online ACP program, PREPARE for YOUR CARE, within subsidized, affordable, and supportive housing. The setting provided a stable environment and existing infrastructure, enabling collaboration with housing specialists and residents to promote ACP in multiple formats (e.g., group and one-on-one) (Pajka et al., 2023). Several implementation barriers were identified in the study, including staff and resident knowledge gaps, inconsistent social support among residents, doubts about the benefits of ACP, and insufficient staff education and authority to implement ACP (Pajka et al., 2023). Conversely, several benefits of the setting and intervention, such as housing stability and user-friendly PREPARE for YOUR CARE materials, provided promising support for continued investigations into these settings to combat the multi-layered insecurity experienced by individuals with low SES experiences.
Addressing Interpersonal Concerns
Family dynamics are crucial to consider when supporting clients, caregivers, and family members throughout the ACP process, particularly when identifying a healthcare proxy and facilitating effective communication. We identified several family-related facilitators and barriers in this review, including supportive and trusted family members; however, family members can also serve as a barrier due to personal or relational factors (e.g., family member topic avoidance). A recent literature review overlapped with some of our findings and captured the complexity of family involvement in ACP for people with advanced cancer. The review revealed that the relationship between two people encompasses at least three domains: the person using ACP, their support person (e.g., a family member or friend), and the nature of their relationship (Kishino et al., 2022). In our review, we identified similar barriers and facilitators, including individual concerns about or optimism for their family member's ACP readiness, family communication patterns that either embraced or avoided ACP, and the presence or absence of mutual respect for autonomy.
Nurses tailor their approach by exploring clients' specific concerns and relational context. We found that individuals with low SES may avoid stressing family members with ACP because of guilt or strained relationships over past stress they caused family members (e.g., asking for loans they did not repay or worrying family members while unhoused). Several co-occurring and severe conditions in low SES communities may contribute to relationship strain and estrangement, such as chronic houselessness, addiction, mental health issues, and previous incarceration (Kaplan et al., 2020). ...individuals with low SES may avoid stressing family members with ACP because of guilt or strained relationships over past stress...
When obtaining secure housing, older adults with a history of chronic houselessness may prioritize repairing relationships; however, this priority may also include avoiding topics that could induce conflict or impose a perceived burden (Padgett et al., 2020). Individual coping and communication styles play a crucial role in involving family members in ACP. Nurses can address family members’ misgivings and emotions and support client-family communication (Kishino et al., 2022). Early ACP topics include providing clients and families with a clear explanation of ACP, addressing any misconceptions, and focusing on what matters most for clients during a health crisis (Izumi, 2017). Additionally, alternative options for support should be available for clients without trusted social support (e.g., completing an advance directive).
Addressing Religious Concerns
We found that religious beliefs were both a facilitator and a barrier in our review, depending on whether clients believed it was their God-given personal responsibility to do ACP or if ACP constituted interference with God’s plans. In the literature, these cultural beliefs and practices are consistent with those found in Black or African American communities (Hong et al., 2018; Sanders et al., 2016; Ward & Montgomery, 2024). Still, as previously discussed, nurses should not discount a client's potential interest in ACP. Often, with some reframing, clients gain a better understanding of what ACP is, its value, and how using ACP can be consistent with their faith practices.
As an example of intervention strategies, faith-based health promotion models have been applied to ACP in African American faith communities, resulting in an increased understanding of reasons why members of those communities may hesitate to do ACP or use hospice (Catlett & Campbell, 2021). Such reasons include differing definitions of a “good death” or suffering, a history of seeing relatives and community members victimized by the healthcare system, and a tradition of using informal or faith-based connections to support loved ones at the end of life (Catlett & Campbell, 2021). Nurses can convey openness to different views about suffering or hospice by letting their clients define what is important to them. Nurses can convey openness to different views about suffering or hospice by letting their clients define what is important to them.
Additionally, healthcare researchers and leaders should collaborate with spiritual leaders and informal faith champions from the outset of an ACP study or program. Community partners provide crucial insight during the planning phase by identifying key players, illuminating site-specific challenges, existing programs that may adopt the initiative, and fostering trusting relationships. Nurses should conduct a thorough review of religious beliefs and practices as part of any ACP conversation to identify important values and preferences regarding care. Additionally, a team-based approach may be most effective by collaborating with chaplains, community faith leaders, and other spiritual representatives to facilitate clients’ religious needs.
Addressing Personal Concerns
Our participants expressed a motivation to engage in ACP to prevent future suffering, and they noted that problem-focused coping styles aligned well with ACP as a proactive measure. Conversely, some of those who desired to avoid stress expressed a desire to avoid ACP. In 2019, the Massachusetts Coalition for Serious Illness Care categorized individuals into action-takers (34%) and non-action-takers (66%), including disengaged worriers, confident independents, and self-reliant skeptics (Massachusetts Coalition for Serious Illness Care, 2019). The group of non-action-takers tended to be more socioeconomically vulnerable, racially and ethnically diverse, and had more challenges with coordinating their health and healthcare activities. Across our studies, we have encountered participants who expressed similar challenges, including fears that their wishes would not be respected, variable trust in healthcare institutions, and numerous social and personal challenges, including challenges to mental health and avoidant coping skills, necessitating mental health perspectives for ACP. ...those who desired to avoid stress expressed a desire to avoid ACP.
Clients with a history of low SES may be at a higher risk for chronic and untreated mental health problems, adverse child and life experiences, fewer protective factors such as supportive familial relationships, and fewer mental health resources (Kirkbride et al., 2024). Avoidant coping may be a coping mechanism that leads to reluctance to engage with ACP in these communities and should be a consideration for nurses as they prepare clients for taking ACP actions (e.g., documentation or discussing preferences with loved ones). Nurses can support clients by considering the whole individual, aligned with the holistic philosophy of nursing. One approach to consider is taking a trauma-informed approach for all clients when broaching ACP topics.
One approach to consider is taking a trauma-informed approach for all clients when broaching ACP topics.Trauma-informed care encompasses six key principles: safety, trust and transparency, peer support, collaboration, empowerment, voice, and choice, as well as consideration of historical, cultural, and gender issues (SAMSHA, 2014). Safety is the first principle, underscoring the need for nurses to foster both psychological and physical safety for one another, as well as their clients in the interpersonal and environmental senses. Fostering safety includes understanding that most people have experienced at least one adverse childhood experience, acting with awareness of the consequences of trauma, and providing care that minimizes and avoids trauma activation and re-traumatization (SAMSHA, 2014). While this approach can be applied to all care types, trauma-informed care is of special interest for approaching ACP with low SES populations. Nursing considerations include assessing clients' privacy preferences, diagnosing any challenges to coping with stress, and developing care plans that align with the participant’s goals.
Conclusion
Nurses are essential advocates and initiators of the ACP process...Communities with low SES are consistently less likely to participate in ACP. Our work has highlighted barriers and facilitators that nurses may consider. Nurses are essential advocates and initiators of the ACP process for clients from diverse backgrounds and are uniquely positioned to fully assess and implement ACP in clinical and community settings. Nurses are trained to regularly consult across disciplines to address complex needs, making hem capable to provide ACP for clients with complex backgrounds and priorities. We have provided several considerations for nurses as they seek to learn more about ACP and provide the best care for their clients.
Authors
Christine C. Kimpel, PhD, RN, MA
Email: kimpel.28@osu.edu
ORCID ID: https://orcid.org/0000-0003-2590-0008
Christine C. Kimpel is an assistant professor at The Ohio State University College of Nursing. She completed a PhD and postdoctoral research fellowship at Vanderbilt University School of Nursing, and a MA in philosophy and BSN at Kent State University. She has extensive experience working with communities with limited income in both clinical and community settings, preparing her to write this manuscript. Her research focuses on increasing advance care planning engagement using trauma-informed intervention approaches and community-engaged implementation strategies.
Cathy A. Maxwell, PhD, RN, FAAN
Email: cathy.maxwell@nurs.utah.edu
ORCID ID: https://orcid.org/0000-0003-1980-8643
Cathy A. Maxwell is a professor at the University of Utah College of Nursing. She earned a BSN and MSN from Troy University and completed a PhD in Nursing Science and postdoctoral fellowship at Vanderbilt University. After serving as a part of the Vanderbilt University, School of Nursing faculty for ten years, she joined the University of Utah College of Nursing. She has earned a reputation as an international expert for the development of evidence-based clinical guidelines for gerontological care and publishing manuscripts regarding advance care planning and aging. She has published extensively and developed interventions that support older adults in understanding their aging trajectory and proactive strategies to support healthy aging.
References
Alvarez, T., & Steffen, B. L. (2021). Worst case housing needs: 2021. https://www.huduser.gov/portal/sites/default/files/pdf/Worst-Case-Housing-Needs-2021.pdf
Amjad, H., Towle, V., & Fried, T. (2014). Association of experience with illness and end‐of‐life care with advance care planning in older adults. Journal of the American Geriatrics Society (JAGS), 62(7), 1304-1309. https://doi.org/10.1111/jgs.12894
Ashana, D. C., D'Arcangelo, N., Gazarian, P. K., Gupta, A., Perez, S., Reich, A. J., Tija, J., Halpern, S.D., Weissman, J.S., & Ladin, K. (2022). "Don't talk to them about goals of care": Understanding disparities in advance care planning. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences, 77(2), 339-346. https://doi.org/10.1093/gerona/glab091
Averill J. B. (2002). Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qualitative Health Research, 12(6), 855–866. https://doi.org/10.1177/104973230201200611
Barwise, A., Juhn, Y. J., Wi, C. I., Novotny, P., Jaramillo, C., Gajic, O., & Wilson, M. E. (2019). An individual housing-based socioeconomic status measure predicts advance care planning and nursing home utilization. The American Journal of Hospice and Palliative Care, 36(5), 362-369. https://doi.org/10.1177/1049909118812431
Blackwood, D. H., Walker, D., Mythen, M. G., Taylor, R. M., & Vindrola-Padros, C. (2019). Barriers to advance care planning with patients as perceived by nurses and other healthcare professionals: A systematic review. Journal of Clinical Nursing, 28(23-24), 4276-4297. https://doi.org/10.1111/jocn.15049
Catlett, L., & Campbell, C. (2021). Advance care planning and end of life care literacy initiatives in African American faith communities: A systematic integrative review. American journal of hospice & palliative medicine, 38(6), 719-730. https://doi.org/10.1177/1049909120979164
Coogan, A., Kimpel, C., Jones, A. C., Barroso, J., Frechman, E., & Maxwell, C. A. (2022). Perspectives on aging and end of life among lower socioeconomic status (SES) older adults. Journal of Applied Gerontology: The Official Journal of the Southern Gerontological Society, 41(6), 1595–1603. https://doi.org/10.1177/07334648221081482
Hickman, S. E., Lum, H. D., Walling, A. M., Savoy, A., & Sudore, R. L. (2023). The care planning umbrella: The evolution of advance care planning. Journal of the American Geriatrics Society (JAGS), 71(7), 2350-2356. https://doi.org/10.1111/jgs.18287
Hong, M., Yi, E. H., Johnson, K. J., & Adamek, M. E. (2018). Facilitators and barriers for advance care planning among ethnic and racial minorities in the U.S.: A systematic review of the current literature. Journal of Immigrant and Minority Health, 20(5), 1277-1287. https://doi.org/10.1007/s10903-017-0670-9
Inoue, M. (2016). The influence of sociodemographic and psychosocial factors on advance care planning. Journal of Gerontological Social Work, 59(5), 401-422. https://doi.org/10.1080/01634372.2016.1229709
Izumi, S. (2017). Advance care planning: The nurse's role. The American Journal of Nursing, 117(6), 56. https://doi.org/10.1097/01.NAJ.0000520255.65083.35
Kaplan, L. M., Sudore, R. L., Cuervo, I. A., Bainto, D., Olsen, P., & Kushel, M. (2020). Barriers and solutions to advance care planning among homeless-experienced older adults. Journal of Palliative Medicine, 23(10), 1300-1306. https://doi.org/10.1089/jpm.2019.0550
Kimpel, C. C., Jones, A. C., Ratcliff, A. C., & Maxwell, C. A. (2022). Affordable housing specialists' perceptions of advance care planning among low-income older adult residents: A qualitative study. Journal of Hospice and Palliative Nursing: JHPN, the Official Journal of the Hospice and Palliative Nurses Association, 24(4), 232–239. https://doi.org/10.1097/NJH.0000000000000870
Kimpel, C. C., Lauderdale, J., Schlundt, D. G., Dietrich, M. S., Ratcliff, A. C., & Maxwell, C. A. (2024). Life-stage and contextual factors of advance care planning among older adults with limited income. Journal of Applied Gerontology: The Official Journal of the Southern Gerontological Society, 43(8), 1144–1155. https://doi.org/10.1177/07334648241230024
Kimpel, C. C., Frechman, E., Chavez, L., & Maxwell, C. A. (2025). Essential advance care planning intervention features in low-income communities: A qualitative study. Journal of Pain & Symptom Management, 69(1), e46–e52. H4.09.018
Kirkbride, J. B., Anglin, D. M., Colman, I., Dykxhoorn, J., Jones, P. B., Patalay, P., Pitman, A., Soneson, E., Steare, T., Wright., T., & Griffiths, S. L. (2024). The social determinants of mental health and disorder: Evidence, prevention and recommendations. World Psychiatry, 23(1), 58-90. https://doi.org/10.1002/wps.21160
Kishino, M., Ellis-Smith, C., Afolabi, O., & Koffman, J. (2022). Family involvement in advance care planning for people living with advanced cancer: A systematic mixed-methods review. Palliative Medicine, 36(3), 462-477. https://doi.org/10.1177/02692163211068282
Massachusetts Coalition for Serious Illness Care (2019). Advancing the language of advance care planning: A messaging research project. https://www.maseriouscare.org/sites/g/files/csphws2481/files/acquiadam-assets/messaging-research-overview-updated-november-2019.pdf.
McMahan, R. D., Hickman, S. E., & Sudore, R. L. (2024). What clinicians and researchers should know about the evolving field of advance care planning: A narrative review. Journal of General Internal Medicine: JGIM, 65(1), e63-e78. https://doi.org/10.1007/s11606-023-08579-5
National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on the Future of Nursing 2020–2030. (2021) Social determinants of health and health equity. In J.L. Flaubert, S. Le Menestrel, D.R.Williams, & M.K.Wakefield (Eds.), The future of nursing 2020-2030: Charting a path to achieve health equity. National Academies Press. https://www.ncbi.nlm.nih.gov/books/NBK573914/ https://doi.org/10.17226/25982
Nouri, S., Lyles, C. R., Rubinsky, A. D., Patel, K., Desai, R., Fields, J., DeRouen, M.C.; Volow, A., Bibbins-Domingo, K., & Sudore, R. L. (2020). Evaluation of neighborhood socioeconomic characteristics and advance care planning among older adults. JAMA Network Open, 3(12), e2029063. https://doi.org/10.1001/jamanetworkopen.2020.29063
Padgett, D. K., Bond, L., Gurdak, K., & Henwood, B. F. (2020). Eliciting life priorities of older adults living in permanent supportive housing. Gerontologist, 60(1), 60-68. https://doi.org/10.1093/geront/gnz040
Pajka, S. E., Kushel, M., Handley, M. A., Olsen, P., Li, B., Enriquez, C., Kaplan, L., & Sudore, R. L. (2023). Using behavioral theory to adapt advance care planning for homeless-experienced older adults in permanent supportive housing. Journal of the American Geriatrics Society (JAGS), 71(8), 2615-2626. https://doi.org/10.1111/jgs.18314
Sanders, J. J., Robinson, M. T., & Block, S. D. (2016). Factors impacting advance care planning among African Americans: Results of a systematic integrated review. Journal of Palliative Medicine, 19(2), 202-227. https://doi.org/10.1089/jpm.2015.0325
Centers for Medicare and Medicaid Services (2025). Advance care planning. Retrieved from: https://www.cms.gov/files/document/mln-advanced-care-planning.pdf
Substance Abuse and Mental Health Services Administration (SAMSHA) (2014). SAMHSA’s concept of trauma and guidance for a trauma-informed approach. https://coresonline.org/sites/default/files/documents/samhsas_concept_of_trauma_and_guidance_for_a_trauma-informed_approach.pdf
Oxford English Dictionary. (n.d.) Stigma. Retrieved from: https://www.oed.com/dictionary/stigma_n?tl=true
Sudore, R. L., Lum, H. D., You, J. J., Hanson, L. C., Meier, D. E., Pantilat, S. Z., Matlock, D.D, Rietjens, J.A.C., Korfage, I.J., Ritchie, C.S., Kutner, J.S., Teno, J.M., Thomas, J., McMahan, R.D., & Heyland, D. K. (2017). Defining advance care planning for adults: A consensus definition from a multidisciplinary delphi panel. Journal of Pain & Symptom Management, 53(5), 821-832. https://doi.org/10.1016/j.jpainsymman.2016.12.331
Ward, C., & Montgomery, K. (2024). End-of-life planning and the influence of socioeconomic status among Black Americans: A systematic review. Journal of Hospice and Palliative Care, 27(1), 21-30. https://doi.org/10.14475/jhpc.2024.27.1.21
Whittle, H. J., Leddy, A. M., Shieh, J., Tien, P. C., Ofotokun, I., Adimora, A. A., Turan, J.M., Frongillo, E.A. Turan, B., & Weiser, S. D. (2020). Precarity and health: Theorizing the intersection of multiple material-need insecurities, stigma, and illness among women in the United States. Social Science & Medicine (1982), 245, 11283. https://doi.org/10.1016/j.socscimed.2019.112683
