


Innovation can be confused with quality improvement (QI), research, and evidence-based practice (EBP) in nursing science, creating conceptual ambiguity that prevents systematic application of an innovation process. This article clarifies innovation as a distinct and rigorous scholarly process, defining it as a verb, a human-centered approach focused on understanding problems and co-creating solutions with end-users, rather than as a product or other outcome. Using design thinking as an example innovation process, we compare innovation to QI, quantitative and qualitative research, and EBP. Key features of innovation include relying on empathy to understand the problem before defining it, employing deliberate divergent thinking, and iterative prototyping with end-users. Each scholarly approach serves a distinct purpose, yet innovation principles can enhance these other processes. We propose that innovation is most appropriate as the primary process when solutions are elusive, when a deep understanding of end-user needs is critical, or when solutions require contextualization. We encourage applying the innovation process to generate patient-centered systems change. This conceptual clarity gives nurse scholars and innovators a framework for better understanding the innovation process compared to other scientific approaches.
Key Words: innovation, quality improvement, evidence-based practice, nursing research, problem solving, design thinking, human-centered design, co-design, healthcare innovation
Innovation has played a critical role in nursing practice throughout history, and contemporary evidence continues to show its impact. Clinically, it has been shown that healthcare institutions that support a culture of innovation are associated with measurable improvements in clinician outcomes, including burnout (O’Hara et al., 2025). Nurses who feel supported by their institutions to innovate are not only more satisfied in their professional roles but are also more likely to engage in innovation activities (Leary et al., 2024). Exposure to innovation activities such as hackathons further builds nurses’ confidence to launch new projects (Kagan et al., 2023). Despite this evidence of positive change, the framework for understanding innovation in nursing science is still developing. While the nursing profession has made significant progress in defining innovation, and professional nursing organizations have created guiding principles and frameworks for innovation (Beaudet et al., 2023; Cámpoli et al., 2025), a gap remains in the deeper conceptualization of innovation in nursing compared to other fields. ...healthcare institutions that support a culture of innovation are associated with measurable improvements in clinician outcomes...
Conceptually, developing this clarity is essential for enhancing the ability of nursing science to systematically study, implement, and evaluate innovative approaches to healthcare delivery and patient care (Kelley, 2023). Innovation is one of several scholarly processes used in nursing, alongside quality improvement (QI), research, and evidence-based practice (EBP), and among these, it remains the least clearly defined and the most often confused with the others (Kelley, 2023). Clarifying what innovation means in relation to QI, research, and EBP is a necessary foundation for systematic innovation in nursing science. Innovation is one of several scholarly processes used in nursing...
Several authors have begun to clarify differences among QI, research, and EBP processes in nursing scholarship (Reynolds et al., 2026). A few have included innovation, working toward useful definitions and differentiation in nursing (Hagle et al., 2020; Keen et al., 2024). Yet, the concept of innovation remains unclear, and the boundaries between the innovation process and other scholarly processes are muddy in practice. Nurse scholars, implementers, and innovators require a clear definition of innovation, an understanding of when to apply the innovation process, and knowledge of how the innovation process and other scholarly approaches complement each other when used in conjunction. In this article, we explore critical definitions and concepts surrounding innovation in nursing practice by highlighting differences, similarities, and applications. ...the boundaries between the innovation process and other scholarly processes are muddy in practice.
Background
Conceptual Foundation of Innovation in Healthcare & Nursing
Innovation in healthcare is a comparatively new field, emerging as a focus area over the last two decades (Kelley, 2023; Leary et al., 2022). Ambiguity around the term "innovation" has led to conflicting definitions and has confused and undervalued its importance in healthcare (Kelley, 2023; Weberg, 2009). Weberg (2009) further argued that innovation requires a convergence of organizational conditions: leadership, financial support, idea generation, teamwork, culture, and demand. Without these conditions, innovators are stifled and innovation stalls.
In nursing and healthcare, as in other fields, innovation has field-specific definitions. The World Health Organization (WHO) defines health innovation as “a fundamental shift in the way countries improve population health and wellbeing not only through information technologies and data science like artificial intelligence, machine learning and telemedicine, but also through social entrepreneurs and others on the ground" (2025, p.1). This definition highlights that innovation is not limited to a specific type of outcome or end product; instead, it encompasses an approach used to understand problems and create solutions. Flessa and Huebner stated that, “In the health care sector, innovations are the source of any improvement in the quality of services and quality of life, but also a steady challenge to existing health care providers and systems” (2021, p. 1). Innovation in healthcare is a comparatively new field, emerging as a focus area over the last two decades
In nursing, innovation has been defined as “the application of creativity or problem-solving that results in a widely adopted strategy, product, or service that meets a need in a new and different way. Innovations are about improvement in quality, cost-effectiveness, or efficiency” (Lachman et al., 2009, p. 205). The American Nurses Association ([ANA], 2024) has established a core “ethos of innovation” to guide innovation in nursing and healthcare, which are largely altruistic and focused on process: “Transparency, democracy, abundance, interprofessional + transdisciplinary collaboration, antiracist + design justice principles (justice, equity, diversity, inclusion), improving the present while being future focused” (p.2). This altruistic ethos sits comfortably within Weberg’s (2009) framing of healthcare innovation as carrying social as well as economic potential, distinguishing it from purely market-driven innovation in other industries. The ANA’s (2024) “need to know” innovation resources endorse several definitions, including the one used by Kelly and Young (2017), who build on E. M. Rogers’ (2003) framing of innovation as “invention + adoption + diffusion.” Kelly and Young (2017) further clarified that the result may be “a novel idea, product, service or care pathway that has clear benefits when compared to what is currently done” (p. 121). ...the word “innovation” can function as both a noun (tangible outcome) and a verb (the process of innovating)
These varied definitions reflect a deeper distinction: the word “innovation” can function as both a noun (tangible outcome) and a verb (the process of innovating) (Fisher, 2020; Kelley, 2023; Merriam-Webster, n.d.). This explains why various definitions focus on process, outcome, or both. There are advantages to conceptualizing innovation as a verb. Fisher (2020) asks us to “consider innovation as a natural act accessible to all” and goes on to hypothesize that “Innovation as a verb; which recognizes that how we do things can be as, or more, important than the results” (para 3).
We align with others (Weberg, 2009; Fisher, 2020) in supporting a process-focused definition of innovation. Our experience indicates that innovation is primarily centered on the human-centered process rather than solely on the final solution (Leary et al., 2024). Notably, throughout this article, we use the term “interestholder” (an individual or group that has an interest in or is affected by the topic) in place of the more common term “stakeholder.” A process-focused definition fosters a collaborative mindset among all interestholders, enabling a shared understanding of the problem and influence of the solution. Among interestholders, end-users are most affected by the outcome, so what matters most is that the end product is co-created with and meets their needs. Ultimately, the process, not just the product, is what transforms healthcare and the people within it.
The Innovation Process
The innovation process occurs when interestholders recognize and understand a problem and work towards a new or adapted solution for the benefit of some part of the organization (Asurakkody & Shin, 2018; Kelley, 2023). The innovation process emphasizes creative idea generation and tailors solutions to improve the environments in which problems affect people (Dy Bunpin et al., 2016; Keen et al., 2024; Purc & Laguna, 2019). There are many innovation processes.There are many innovation processes. We focus here on design thinking (DT) and related concepts because they are more accessible for beginners to understand and apply, and they have demonstrated applicability in healthcare settings when used by nurses (Leary et al., 2022).
Innovation, human-centered design (HCD), and DT are distinct concepts operating at different scales within the innovation process. Innovation is a broad approach. HCD is one framework for operationalizing it, and DT is a specific structured process within HCD. In this article, we use DT as our exemplar innovation process. HCD is a methodological framework for addressing complex problems and developing solutions that prioritize and respond to the needs and perspectives of the intended users and interestholders (Leary et al., 2022; IDEO, 2025).
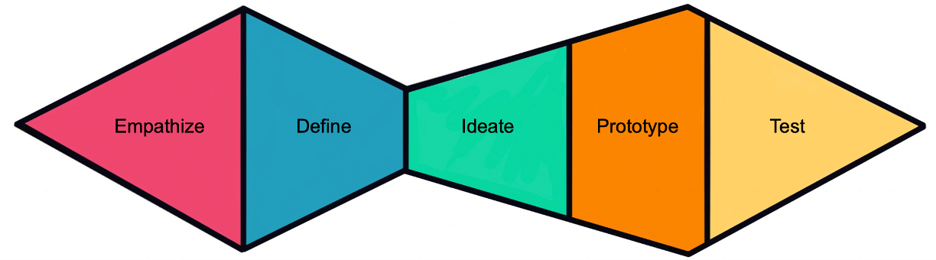
HCD focuses on incorporating interestholders in meaningful collaboration throughout each phase of the process. HCD uses DT to rigorously understand end-user needs, wants, and desires through a 5-stage process: empathizing, defining, ideating, prototyping, and testing (Interaction Design Foundation, n.d.; Leary et al., 2022). The DT process is situated within the double-diamond approach of divergent and convergent thinking (see Figure).
Figure. The Five Stages of the Innovation Process of Design Thinking, which are Iteratively Implemented in Practice
(AUTHORS: Can we add a citation for this figure? IDF or Leary et al., 2022 maybe? If the figure is published elsewhere first, we will need permission to reprint it from that publisher – an email that you forward to me is sufficient. Otherwise, if it has not been previously published we can just cite the work where the five stage process is discussed. Thanks! Jackie)
Although the DT process is depicted linearly, it is implemented iteratively and designed to be executed by a team. The Design Thinking for Health (2025) training site describes each step of the process. For example, empathy involves consistently returning to the end-user’s needs and underlies the entire process. Defining is a convergent process that guides the team in describing the problem sufficiently to understand it, while purposefully refraining from including a solution in the definition. Ideation is a divergent process that may involve brainstorming, where all ideas are welcomed, and the team intentionally considers various options, pushing beyond the first few solutions that come to mind. The team iteratively creates prototypes of the solutions, testing them with end-users in increasingly sophisticated ways. Early prototypes are intentionally low-fidelity, or basic, to gather feedback before the team becomes too set in a solution. Ideation is a divergent process that may involve brainstorming, where all ideas are welcomed...
A fourth concept, equity-centered design (ECD) operates as a justice-oriented overlay across both HCD and DT. ECD requires teams to acknowledge their assumptions and biases, the power dynamics within end-user groups, and the systemic biases that exist in systems, while also ensuring that the history and lived experiences of the populations for whom they are designing are centered throughout (Creative Reaction Lab, n.d.). Together, HCD, DT, and ECD form a layered system: HCD as the framework, DT as the method, and ECD as the justice overlay. Although it may seem straightforward, DT and HCD are conceptualized and applied with considerable variability (Leary et al., 2022). This variability highlights the importance of clearly situating the innovation process within the broader landscape of nursing scholarly approaches.
Existing Models: I3 and INQUIRE Models
Hagle et al. (2020) reported on the I3 Model for Advancing Quality Patient Centered Care, which provides an algorithm to help nurses differentiate among innovation, QI, and inquiry (research & EBP). The authors describe innovation as beginning with the question, “Is there a new way?” In contrast, QI initiatives start with questions like "Is there a better way?" and research and EBP ask, “Why are we doing it this way?” (Hagle et al., 2020, Supplemental Digital Content). According to the I3 model, the innovation process requires a deep understanding of the problem that the population of focus is experiencing, achieved through curiosity. Once the problem is understood, the team develops a plan and prototype, shares it with stakeholders, pilots the solution, and evaluates the results.
The I3 model notes that the QI process often employs techniques such as the model for improvement (Langley et al., 2009) and that the research process involves defining a methodology, obtaining Institutional Review Board (IRB) approval for safe data collection, and disseminating the findings. According to the I3 model, EBP involves gathering the best evidence to make practice recommendations. Moreover, an important difference is that innovation includes a discovery step that drives deeper understanding of the problem after it is defined; a step not present in the EBP, QI, or research arms of the model. Scholars use these characteristics, which are part of the corresponding I3 model algorithm, to determine when to use each type of scholarly process. ...an important difference is that innovation includes a discovery step that drives deeper understanding of the problem after it is defined...
The INQUIRE (INnovation, QUality Improvement, Research, and Evidence-Based Practice) model and algorithm were iteratively developed and tested to aid clinicians and nurse scholars to discern a process that aligns with their project and solution options (Keen et al., 2024). The authors recommended all a stepwise process beginning with noticing a "trigger", then studying it and looking for solutions, evidence, or implementable practices. The INQUIRE-associated toolkit worksheet (Keen et al., 2024, Supplemental Digital Content) suggests that when sufficient evidence or established practice exists, the user moves to implementation, choosing QI for a process change or EBP for a practice change. The toolkit further clarifies that a gap in the literature or an intent to generate new knowledge should trigger the use of the research process. Keen et al. (2024) suggest that innovation is appropriate when evidence is absent, when available evidence does not fit the environment, or when an evidence-based solution has failed.
Differentiating the Innovation Process from Other Approaches in Nursing Science
The I3 and INQUIRE models offer important pathways for selecting among innovation, QI, research, and EBP, but neither examines what the innovation process actually involves at a methodological level. We add two conditions where an innovation process serves teams better: when understanding end-user needs deeply is essential, and when the solution must be contextualized to a specific setting or population. We build on these models by examining a specific innovation process, DT, and comparing its methods, mindset, and outputs to exemplar QI, research, and EBP processes.
Comparing Across Approaches
We examined exemplar approaches from each process: DT for innovation, the Institute for Healthcare Improvement (IHI) Model for Improvement for QI, Flanagan and Beck's research process, and the Johns Hopkins model for EBP. Innovation distinguishes itself among these approaches by treating the process itself as transformative, not solely the resulting solution. These exemplars do not represent the full range of approaches within each scholarly process, but they illustrate key differences among the four and opportunities for integration. We discuss each comparison in turn, beginning with QI (also see Table).
Table. A Comparison of Aims, Exemplar Process, and Outcomes by Nursing Scholarly Processes
|
Aim |
Exemplar Process |
Outcome |
|
|---|---|---|---|
|
Innovation |
Generate a new solution to an unmet need |
Design thinking - Empathize, define, ideate, prototype, & test (Design Thinking for Health, 2025). |
A new product, process, or service adopted to address a need. |
|
Quality Improvement |
Process change based on local data |
IHI model for improvement - Understand the issues with three fundamental questions, then iteratively Plan-Do-Study-Act (Langley et al., 2009). |
Studied localized change |
|
Research, Quantitative |
Create generalizable knowledge |
Conceptualization, design, and planning, focusing on empirics (collecting/prepping data), analysis, and dissemination (Flanagan & Beck, 2025) |
Generalizable knowledge |
|
Research, Qualitative |
Exploration or interpretation of human experience |
Plan the study, iteratively develop data collection strategies & gather/analyze evidence, and disseminate findings (Flanagan & Beck, 2025) |
Understanding, theory, hypothesis |
|
Evidence-Based Practice |
Use high-quality knowledge to inform practice |
Johns Hopkins EBP model - Cyclical and reflective process of inquiry, practice question, evidence, translation, best practices, & practice improvements (Bissett et al., 2025) |
Assessed evidence-based change |
Innovation Compared to QI. One example of a QI process is the IHI model for improvement (Langley et al., 2009). In this QI process, a team forms and asks three fundamental questions about the project goals: what aims need to be set, what change is needed, and how the change will be measured (Langley et al., 2009). The project then progresses through a cycle of expanding changes from small to large scale. The change is planned and tested, with results observed and lessons learned implemented on a small scale before the process restarts and expands to a larger scale following the Plan-Do-Study-Act (PDSA) cycle. The process is often augmented by other QI tools such as fishbone diagrams and process maps to deepen problem understanding (Tagaram & Chen, 2025). One example of a QI process is the IHI model for improvement.
Using the model for improvement as an example, we identify several similarities and differences between innovation and QI. Both approaches require a planning process before implementation. However, the model for improvement process has a different starting point than DT. The planning phase of the IHI process includes asking three key questions but does not include purposeful divergent thinking (Langley et al., 2009). While multiple solutions can be considered during planning, there is no structured brainstorming step. By comparison, DT focuses on empathizing with the needs of all interestholders to understand the problem, encourages divergent thinking about potential solutions, and selects the most suitable change in collaboration with end-users. Importantly, the IHI process begins with a definition phase, having already identified the problem to solve, whereas DT begins with the empathy (or understanding) phase. This distinction is reflected in the I3 model algorithm, which places goal-setting at the start of the Improvement arm and a separate discovery step within the Innovation arm (Hagle et al., 2020). QI explicitly requires clear measures and aims to be established early, which is a strength. DT, by contrast, works to understand the problem from the end-users' perspective and incorporates their insights before considering solutions (Beaird et al., 2018).
Both the PDSA cycles and DT are iterative in nature, starting with small changes that are tested and then expanded, although the iteration styles differ. DT embraces a more fluid and iterative process, returning regularly to the perspectives of end-users and other interestholders. In contrast, the QI process is cyclically iterative, typically progressing through planning, doing, studying, and acting before repeating the cycle. Innovation and QI are similar in that both processes lead to a change. Neither results in generalizable knowledge (Keen et al., 2024). Innovation and QI are similar in that both processes lead to a change.Research, by contrast, aims to generate knowledge that travels beyond a single context; we examine DT alongside Flanagan and Beck's (2025) quantitative and qualitative research processes next.
Innovation Compared to Research. “Nursing research is designed to generate evidence about issues important to the delivery and outcomes of patient care" (Flanagan & Beck, 2025, p. 2). Quantitative research follows the steps of the scientific method, employing clear and systematic procedures to create generalizable knowledge (Keen et al., 2024). The phases of the scientific method within a positivist framework include conceptualization, design and planning, empirical data collection and preparation, analysis, and dissemination (Flanagan & Beck, 2025).
There are parallels between DT and the quantitative process described by Flanagan and Beck (2025). Both involve testing, but they differ in approach. During the DT testing phase, the team tests a low-fidelity prototype with end-users. This phase is not intended to generate generalizable knowledge; rather, it ensures that the solution meets end-user needs and addresses the defined problem (Keen et al., 2024). Moreover, testing occurs repeatedly in the DT process, starting with a low-fidelity prototype and progressing to a minimally viable product. Quantitative research, in contrast, generates knowledge that is generalizable to broader populations. The process is carefully planned, and the exact steps are approved by an institutional review board (IRB), leaving little room for change once underway (Hagle et al., 2020). Thus, while both DT and quantitative research involve testing, the nature of that testing differs substantially. Other differences exist beyond testing, such as the absence of an explicitly divergent step in the quantitative research process. The qualitative process is the only other nursing scholarly approach that emphasizes divergent thinking as innovation does.
Qualitative research explores concepts or experiences from a constructivist perspective, seeking to understand experiences or generate ideas, such as theories (Flanagan & Beck, 2025). Flanagan and Beck’s qualitative research follows the steps of planning the study, iteratively developing data collection strategies, gathering and analyzing evidence, and disseminating findings. Both DT and Flanagan and Beck's qualitative research address the human experience and use similar techniques, such as interviews and observations, to collect data. DT explicitly aligns itself with ethnographic methods, a specific type of qualitative research, and aims to understand the experience of interestholders. Yet their outcomes differ. Whereas qualitative processes typically strive to describe the human experience and perhaps use it to develop theory or subsequent hypotheses, DT uses it to develop human and equity-centered solutions. DT draws on qualitative research principles, such as using data saturation as an indicator for transitioning from empathy to defining a problem and again when garnering feedback during the prototyping and testing phases. The qualitative process is the only other nursing scholarly approach that emphasizes divergent thinking as innovation does.
Both research and innovation aim to fill a gap; however, research seeks to address a knowledge gap, while innovation aims to provide a solution (Keen et al., 2024). Research can also be viewed as a broader process that extends beyond individual studies, encompassing all research related to a particular topic. This process iteratively progresses through both qualitative and quantitative processes, typically beginning with qualitative research when little is known about a topic. Viewed as a larger program of inquiry rather than a single study, research cycles through phases similar to DT, moving from open exploration through qualitative work to more structured testing through quantitative methods. In this broader sense, research more closely resembles innovation. EBP, by contrast, draws on existing evidence rather than generating new knowledge or solutions. We compare this to DT next, using the Johns Hopkins EBP model.
Innovation Compared to Evidence-Based Practice. Dang et al. (2022) defined EBP as “a problem-solving approach to clinical decision-making within a healthcare organization” (p.5). EBP integrates the best available scientific evidence with experiential evidence from patients and practitioners and is useful when a clinician’s question can be addressed by existing literature (Bissett et al., 2025; Keen et al., 2024). The Johns Hopkins Evidence-Based Practice (JHEBP) model, a commonly used framework, organizes EBP into three components (inquiry, practice, and learning) that occur within a collaborative, often interprofessional, context (Bissett et al., 2025). Like DT, the JHEBP model is iterative, allowing teams to revisit and revise earlier components based on new insights. DT relies on divergent thinking, where varied perspectives expand the range of possible solutions.
The information collected during the inquiry phase informs the practice component of the JHEBP model, which follows a stepwise process called PET: practice question, evidence, and translation (Bissett et al., 2025). In the practice question step, the team investigates the clinical problem to craft a focused statement narrow enough to guide an evidence search (Bissett et al., 2025, p. 28). DT, by contrast, frames problem statements broadly so they do not constrain solutions in advance. The divergent thinking of DT depends on keeping the problem statement open. The two processes also draw on different evidence and different kinds of diversity. During the JHEBP model’s evidence step, the team searches, summarizes, organizes, and synthesizes academic literature to recommend best practice (Bissett et al., 2025). DT, in contrast, treats interestholders, particularly end-users, as primary sources of insight from the start. The JHEBP model relies on interprofessional teams to interpret and apply evidence. DT relies on divergent thinking, where varied perspectives expand the range of possible solutions.
In the JHEBP model, the translation phase involves assessing how the best-evidence recommendations align with practice, considering feasibility, and identifying associated risks (Bissett et al., 2025). Teams develop recommendations and an action plan for the practice setting, then implement and study the practice improvement. DT, by comparison, starts with brainstorming, then moves into iterative cycles of prototyping and testing. These cycles refine the solution and deepen understanding of the problem. Both processes end by gathering data on what worked. The JHEBP model offers a clear, stepwise pathway when the evidence is established and the goal is to apply it. DT is more useful when the problem is not yet well understood or when no evidence-based solution exists (Keen et al., 2024).
Integrating Innovation Principles into QI, Research, and EBP
What Innovation Principles Can Offer Other Scholarly Processes
While the preceding sections established innovation as a distinct scholarly process, its principles can also enhance QI, research, and EBP when used in combination. Empathizing with interestholders, cycles of divergent and convergent thinking, and prototyping can all be integrated into these approaches, and have been recognized as valuable in healthcare settings (Ku & Lupton, 2020).
As clinicians, we typically use nursing scholarly processes to inform healthcare changes, assuming we already understand the problems our patients or communities face (Beaird et al., 2018). Sometimes that assumption holds, but the innovation process makes clear that we need deeper contextual understanding through insights from end-users in their own settings. Strategies for gaining empathy help us catch what we might otherwise miss, both subtle and overt. Consider a team addressing frequently missed follow-up appointments. QI might measure and reduce no-show rates, EBP might identify evidence-based scheduling interventions, and research might study predictors of non-attendance. An innovation approach would first seek to understand patients’ lived experiences of the barriers before defining the problem or proposing solutions. To do this, DT uses techniques like interviewing interestholders, observing end-user experiences, and exploring parallel experiences (e.g., trying the hospital check-in process you are changing) to better understand problems and develop solutions (Design Thinking for Health, 2025). ...the innovation process makes clear that we need deeper contextual understanding through insights from end-users in their own settings.
Co-design extends empathy by inviting interestholders to actively participate in the design process (Ku & Lupton, 2020). Strategies for empathy and co-design can be incorporated into other scholarly processes. For instance, including patients in the planning of a QI effort can sharpen the team’s understanding of the problem and surface whether potential solutions are useful from the end-user perspective. Healthcare has made real progress in patient-centered care, responding to individual patient needs in clinical interactions. Innovation offers a scholarly method for addressing problems at the systems level, where the work is no longer about responding to one patient at a time but about reshaping the conditions that affect many.
Brainstorming is a technique for engaging in divergent thinking. In a brainstorming session, all ideas are valid, and the team is encouraged to push past the first few suggestions that come to mind (Ku & Lupton, 2020). The underlying principle is simple: the first idea is rarely the best one, and a wider field of options gives the team more to work with. Brainstorming could strengthen the early phases of other processes, including QI planning, the inquiry stage of quantitative research, and the inquiry phase of EBP, by broadening the range of solutions a team considers. ...the first idea is rarely the best one, and a wider field of options gives the team more to work with.
Prototypes are tangible representations of an idea, often visual and deliberately rough at first, designed to gather feedback before a team commits to a direction (Ku & Lupton, 2020). Innovators build prototypes early and revise them as they learn, treating each version as something to test rather than defend (Design Thinking for Health, 2025). The same approach can extend to other nursing scholarly processes. Researchers can build a low-fidelity mock-up of a survey instrument or recruitment flow and get feedback before using it. QI teams can sketch a workflow change on paper and walk through it with staff before testing it on a unit. EBP teams can develop draft visual aids for an implementation plan and review them with frontline nurses before rolling the plan out.
Across empathy, brainstorming, and prototyping, the underlying innovation principle is the same: scholarly work in nursing is strengthened when teams hold their own assumptions lightly. The first understanding of the problem may miss something important; the first solution may not be the best; the first design may not survive contact with end-users. Innovation principles offer concrete techniques for catching these gaps in QI, research, and EBP, where the temptation to confirm an existing plan can quietly shape outcomes. These principles can be taught; graduates of interdisciplinary innovation courses report continuing to apply teamwork, innovation, and learning skills in their professional work (Lewis et al., 2023). Innovators build prototypes early and revise them as they learn...
Practical Considerations
Borrowing a technique from another scholarly process does not transform the work into that process. Sandelowski (2000), when writing about qualitative descriptive research, made a similar argument: borrowing techniques from other qualitative traditions does not transform a qualitative descriptive study into something else. The same logic applies across scholarly processes more broadly. Each approach retains its unique purpose, standards, and outcomes, and integrating ideas from another approach does not make the approaches equivalent. For example, a researcher who interviews end-users while generating a hypothesis is borrowing an empathy-building technique from DT, but the project is still research, not innovation. Borrowing a technique from another scholarly process does not transform the work into that process.The researcher should describe a clear research process and note that it was augmented with techniques to build empathy. Naming what the project actually is, and what was borrowed, keeps the rigor of each approach intact.
IRBs play an important role in protecting research participants, but traditional IRB processes are designed primarily for linear research, where the protocol is fixed in advance. Innovation work rarely fits that mold. The same is true of qualitative research, where planning and analysis often unfold together rather than in sequence (Flanagan & Beck, 2025). Yet, IRBs have developed ways to accommodate that iterative work. Similar flexibility could support innovation: a staged approval process, for example, or approving an initial plan with the expectation that the team will return as the work evolves. Innovators who plan to publish their findings, including quotes or data from interestholders, can work with their IRBs to balance flexibility with participant protection. Signed consent requirements, for instance, may be waived if the team keeps only anonymous notes. As innovation becomes more established as a scholarly process in nursing, IRB structures will need to evolve alongside it.
Conclusion
We compared the innovation process to QI, research, and EBP, clarifying what makes innovation distinct as a scholarly process and showing how its principles can augment the other approaches. We argued that innovation is process-centered: it prioritizes empathy with interestholders, divergent and convergent thinking, and iterative prototyping with end-users. Building on the I3 and INQUIRE models, we proposed conditions where an innovation process serves teams better, when understanding end-user needs deeply is essential and when a solution must be contextualized to a specific setting or population. We also showed that innovation principles can be incorporated into QI, research, and EBP without blurring the distinctions among them, sharpening each process while preserving its rigor. More work is needed to document innovation processes in nursing practice, evaluate their outcomes, and prepare nurses to innovate.
Authors
Erica J. Lewis, PhD, RN
Email: Lewisej@jmu.edu
ORCID ID: 0000-0002-5294-7517
Erica J. Lewis is a Professor at James Madison University School of Nursing with expertise in innovation pedagogy and interdisciplinary education. She has led the integration of design thinking into nursing education, developing and teaching multiple innovation courses across all levels of nursing education. She has presented nationally and internationally on applying human-centered design approaches to healthcare and educational challenges.
Marion Leary, PhD, MPH, RN
Email: mleary@nursing.upenn.edu
ORCID ID: 0000-0002-4815-4223
Marion Leary is the Director of Innovation at the University of Pennsylvania School of Nursing. Dr. Leary is an expert in innovation methodology, studying human-centered design, equity-centered design, and design thinking in healthcare and nursing. Dr. Leary teaches courses, performs research, and directs programs specific to the innovation process.
References
American Nurses Association. (2024). iac American Nurses Association innovation: Need to know innovation resources. Retrieved from: https://www.nursingworld.org/globalassets/innovation/guide/iac-general-innovation-resources_2024-q1-updates_final.pdf
American Nurses Association. (n.d.). Innovation guide. Retrieved from: https://www.nursingworld.org/practice-policy/innovation/innovation-guide/
Asurakkody, T. A., & Shin, S. Y. (2018). Innovative behavior in nursing context: A concept analysis. Asian Nursing Research, 12(4), 237–244. https://doi.org/10.1016/j.anr.2018.11.003
Beaird, G., Geist, M., & Lewis, E. J. (2018). Design thinking: Opportunities for application in nursing practice. Nurse Education Today, 64, 115–118.
Beaudet, O., Pesut, D., & Lemberger, O. (2023). The ANA innovation engine: Activating innovation through education and communities of practice. OJIN: The Online Journal of Issues in Nursing, 28(2). https://doi.org/10.3912/OJIN.Vol28No02Man03
Bissett, K., Ascenzi, J., & Whalen, M. (2025). Johns Hopkins evidence-based practice for nurses and healthcare professionals: Models & guidelines (5th ed.). Sigma Theta Tau International.
Cámpoli, M., Mulvey, T., Lemberger, O., Person, H., Bellegarde-Armstrong, K., & Beaudet, O. (2025). A pilot study to create a culture of innovation and quality: Focus on a nursing association, credentialing center, and foundation. Nursing Reports, 15(9), 313. https://doi.org/10.3390/nursrep15090313
Creative Reaction Lab (CRXLab). (n.d.). Our approach: Equity-centered design. Retrieved from: https://crxlab.org/our-approach
Dang, D., Dearholt, S. L., Bissett, K., Ascenzi, J., & Whalen, M. (2022). Johns Hopkins evidence-based practice for nurses and healthcare professionals: Model and guidelines (4th ed.). Sigma Theta Tau International.
Design Thinking for Health. (2025). Design Thinking for Health. Retrieved from: https://designthinkingforhealth.org/
Dy Bunpin, J. J., 3rd, Chapman, S., Blegen, M., & Spetz, J. (2016). Differences in innovative behavior among hospital-based registered nurses. The Journal of Nursing Administration, 46(3), 122–127. https://doi.org/10.1097/NNA.0000000000000310
Fisher, B. (2020, March 1) Innovation as a verb. Forbes. https://www.forbes.com/sites/billfischer/2020/03/01/innovation-as-a-verb/
Flanagan, J. & Beck, C.T. (2025). Polit & Beck’s Nursing Research: Generating and Assessing Evidence for Nursing Practice (12th ed.). Wolters Kluwer.
Flessa, S., & Huebner, C. (2021). Innovations in Health Care - A Conceptual Framework. International Journal of Environmental Research and Public Health, 18(19), 10026. https://doi.org/10.3390/ijerph181910026
Hagle, M., Dwyer, D., Gettrust, L., Lusk, D., Peterson, K., & Tennies, S. (2020). Development and implementation of a model for research, evidence-based practice, quality improvement, and innovation. Journal of Nursing Care Quality, 35(2), 102–107. https://doi.org/10.1097/NCQ.0000000000000422
IDEO. (2025). Design kit: The human-centered design toolkit. Retrieved from: https://www.ideo.com/journal/design-kit-the-human-centered-design-toolkit
Interaction Design Foundation. (n.d.). Design thinking. Retrieved from: https://www.interaction-design.org/literature/topics/design-thinking
Kagan, O., Sciasci, N. G., Koszalinski, R. S., Kagan, D. H., Leary, M., & Nadel, H. (2023). Nurses' confidence in starting a new venture, startup, or project in the context of nurse-led hackathons: Results of a prehackathon survey. Nursing Outlook, 71(3), 101961. https://doi.org/10.1016/j.outlook.2023.101961
Keen, A., Radecki, B., Snyderman, W., Rader, T., Hemmelgarn, A., & Sierp, A. (2024). INnovation, QUality Improvement, Research, and Evidence-Based Practice (INQUIRE): A navigation model for change and discovery. Journal of Nursing Care Quality, 39(1), 18–23. https://doi.org/10.1097/NCQ.0000000000000724
Kelley, T. F. (2023). Advancing the nursing profession through innovation. In S. Xavier & L. Nunes (Eds.), Nursing: Trends and developments (5th ed.). IntechOpen. https://doi.org/10.5772/intechopen.110704
Kelly, C. J., & Young, A. J. (2017). Promoting innovation in healthcare. Future Healthcare Journal, 4(2), 121–125. https://doi.org/10.7861/futurehosp.4-2-121
Ku, B., & Lupton, E. (2020). Health design thinking: Creating products and services for better health. MIT Press.
Lachman, V. D., Glasgow, M. E. S., & Donnelly, G. F. (2009). Teaching innovation. Nursing Administration Quarterly, 33(3), 205-211. https://doi.org/10.1097/NAQ.0b013e3181acca9a
Langley, G. L., Moen, R., Nolan, K. M., Nolan, T. W., Norman, C. L., & Provost, L. P. (2009). The improvement guide: A practical approach to enhancing organizational performance (2nd ed.). Jossey-Bass.
Leary, M., Cacchione, P. Z., Demiris, G., Carthon, J. M. B., & Bauermeister, J. A. (2022). An integrative review of human-centered design and design thinking for the creation of health interventions. Nursing Forum, 57(6), 1137-1152.
Leary, M., Demiris, G., Brooks Carthon, J. M., Cacchione, P. Z., Aryal, S., & Bauermeister, J. A. (2024). Determining the innovativeness of nurses who engage in activities that encourage innovative behaviors. Nursing Reports, 14(2), 849–870. https://doi.org/10.3390/nursrep14020066
Lewis, E. J., Ludwig, P. M., Arce-Trigatti, A., Geist, M., Kurti, S. P., Nagel, J., & Sanders, R. (2023). Persistent outcomes for college graduates who completed an innovation course, Journal on Excellence in College Teaching, 34(1). Retrieved from: https://celt.miamioh.edu/index.php/JECT/article/view/144
Merriam-Webster. (n.d.). Innovation. In Merriam-Webster.com dictionary. Retrieved from: https://www.merriam-webster.com/dictionary/innovation
O'Hara, S., Melnyk, B. M., Hsieh, A. P., Helsabeck, N. P., Giuliano, K. K., & Vital, C. (2025). Innovation, wellness, and EBP cultures are associated with less burnout, better mental health, and higher job satisfaction in nurses and the healthcare workforce. Worldviews on Evidence-Based Nursing, 22(2), e70012. https://doi.org/10.1111/wvn.70012
Purc, E. & Laguna, M. (2019). Personal values and innovative behavior of employees. Frontiers in Psychology, 10, 865. https://doi.org/10.3389/fpsyg.2019.00865
Reynolds, S. S., Waldrop, J. B., & Dunlap, J. J. (2026). Appropriate use of evidence-based practice quality improvement and research methods, designs, and terminology: Understanding the differences. Journal of Nursing Care Quality, 41(1), 1–6. https://doi.org/10.1097/NCQ.0000000000000890
Rogers, E. M. (2003). Diffusion of Innovations (5th ed.). Free Press.
Sandelowski, M. (2000). Whatever happened to qualitative description? Research in Nursing & Health, 23(4), 334-340.
Tagaram, S. D., & Chen, C. (2025). Quality tools and techniques: Fishbone diagram, Pareto chart, process map. In StatPearls. StatPearls Publishing.
Weberg D. (2009). Innovation in healthcare: A concept analysis. Nursing AdministrationQuarterly, 33(3), 227-237. https://doi.org/10.1097/NAQ.0b013e3181accaf5
World Health Organization. (2025). Innovation for health impact. Retrieved from: https://www.who.int/westernpacific/initiatives/innovation-for-health-impact