


The Nursing Now! campaign, a program of the Burdett Trust for Nursing, is being undertaken in collaboration with the World Health Organization and the International Council of Nurses to create a social movement to improve health globally by raising the profile and status of nurses worldwide. Recently, the Nursing Now! campaign produced a report that was launched at the 2018 WISH Foundation meeting in Qatar that explored how the profession of nursing could contribute to the rapid and cost-effective expansion of high-quality universal health coverage (UHC). In this research study we identified how nurses, relative to the medical profession, are contributing to scholarship on UHC, and explored potential opportunities to leverage already-published research toward this agenda. This article offers background and history about UHC, and discusses the methods, results, recommendations, and limitations of our study. The profession of nursing lags significantly behind the medical profession but can potentially make rapid progress if the isolated efforts of researchers are harnessed and systematic methods of knowledge transfer are applied to existing research on nurse-led services and directed toward the pursuit of UHC. This study establishes a baseline of current nursing scholarship that can be used to assess progress in addressing today’s policy opportunities.
Key Words: Nursing Now!, universal health coverage, nurse-led services, Sustainable Development Goals, bibliometrics
The 33rd President of the United States (U.S.), Harry Truman, in his oral biography said, “There is nothing new in the world apart from the history you do not know” (Miller, 1974). Far earlier, Florence Nightingale, in her 1872 addresses to probationers and qualified nurses, said “For us who nurse, our nursing is a thing, which, unless we make progress every year, every month, every week, take my word for it we are going back” (Nash, 1914). It is our intention to use the concepts contained within these two quotes – learning from history and the need to make progress – as the synergistic drivers to explore the opportunities that the nursing profession now faces.
The [Nursing Now!] campaign seeks to improve health globally by raising the profile and status of nurses worldwide...As we approach the 200th anniversary of the birth of Nightingale, the Nursing Now! Campaign (WHO, n.d.a) is preparing to use this auspicious event as a springboard to the future. The campaign is a program of the Burdett Trust for Nursing (n.d.) and is being undertaken in collaboration with the World Health Organization (WHO, n.d.b) and the International Council of Nurses (ICN, n.d.). The campaign seeks to improve health globally by raising the profile and status of nurses worldwide – influencing policymakers and supporting nurses themselves to lead, learn and build a global movement. Centered on five objectives (Table 1), Nursing Now! continues to mobilize international partners, as well as more than 60 national nursing groups.
Table 1. Nursing Now! Objectives and Goals
|
Objective |
Detail and Goals |
|
1 |
Greater investment in improving education, professional development, standards, regulation and employment conditions for nurses.
|
|
2 |
Increased and improved dissemination of effective and innovative practice in nursing.
|
|
3 |
Greater influence for nurses and midwives on global and national health policy, as part of broader efforts to ensure health workforces are more involved in decision-making.
|
|
4 |
More nurses in leadership positions and more opportunities for development at all levels.
|
|
5 |
More evidence for policy and decision makers about: where nursing can have the greatest impact, what is stopping nurses from reaching their full potential and how to address these obstacles.
|
It is not possible in a single article to address all the objectives set out by the campaign. Instead, we focus on the pursuit of universal health coverage (UHC) and, when appropriate in our critique of how this can be attained, simultaneously address other objectives. Our research identified how nurses, relative to the medical profession, are contributing to scholarship on UHC, and explored potential opportunities to leverage already-published research toward this agenda. This article offers background and history about UHC, and discusses the methods, results, recommendations, and limitations of our study.
Background
Universal health coverage came to prominence as part of the deliberations on the then Millennium Development Goals...Recently, as part of the World Innovation for Health Summit, Nursing Now! released a report exploring how nurses could contribute to the rapid and cost-effective expansion of high-quality UHC (Crisp, Brownie, & Refsum, 2018). Universal health coverage (The World Bank, n.d.) came to prominence as part of the deliberations on the then Millennium Development Goals (MDGs) and was subsequently integrated into discourse on pursuit of the Sustainable Development Goals (SDGs; United Nations, 2015). Research has shown that nursing was late to address the opportunities presented in pursuing the MDGs but has a more promising start with the SDGs (Benton & Shaffer, 2016). Benton and Shaffer (2016) argued that nurses have a wide range of potential contributions to make across all 17 of the SDGs but they noted that the initial focus of the profession was extremely narrow, limiting scholarly activity to targets relating to a small subset of the SDGs.
...nurses need to come to the table prepared to provide evidence rather than opinion.Benton, Pérez-Raya, Fernandez-Fernandez, & González-Jurado (2015) identified that with today’s increased need to support policy change with graded evidence, nurses need to be more active in generating, curating and presenting robust, reliable and valid research to influence the direction of change. Benton, Al Maaitah, & Gharaibeh (2017) further argued that if the profession of nursing’s policy voice is to be heard by the WHO, the World Bank Group, and other intergovernmental agencies, then nurses need to come to the table prepared to provide evidence rather than opinion.
Relying on one-off exemplars or unpublished reports is totally inadequate if the criticisms levied by Oxman, Lavis, & Fretheim (2007) of the WHO policy-making process are to be addressed. While case studies, such as those cited in the report by Crisp et al. (2018), are interesting and offer a glimpse of the potential contribution of the profession to the pursuit of UHC, they are insufficient to meet the requirements of evidence as set out in the WHO handbook for guideline development (2012). To make a quantifiable difference and gain wide-scale support for systemically implementing such exemplars, more robust, reliable and valid evidence is required.
The Historical Context of Nightingale and Universal Health Coverage
Distressed by her observations, Nightingale is perhaps one of the first proponents of delivering UHC to a population. In the midst of the mayhem of the Crimean War, she saw the need for sanitation, nutrition and essential care. Conscious that the absence of these fundamental requirements killed more troops than the injuries inflicted by the enemy, she gathered data to mobilize opinion and resources to address this terrible and unjust situation. Today, even in the absence of war, populations are often confronted with a lack of access to essential health services as well as a wide range of burdens originating from what is now known as the ‘social determinants of health’ (Nicholson, Yates, Warburton, & Fontana, 2015; WHO, 2018).
Indeed, so successful was she as a change agent that she is, for many around the world, acknowledged as the progenitor of modern nursing.Nightingale was well educated, an excellent communicator, and connected to eminent and influential leaders of the day, so was able to mobilize resources to bring about change (River, 2018). Indeed, so successful was she as a change agent that she is, for many around the world, acknowledged as the progenitor of modern nursing. Yet for others, she is seen as a founding pioneer in the application of statistics and data visualization, and a formidable advocate of the public health revolution (Small, 2017).
Figure 1. Polar Diagram
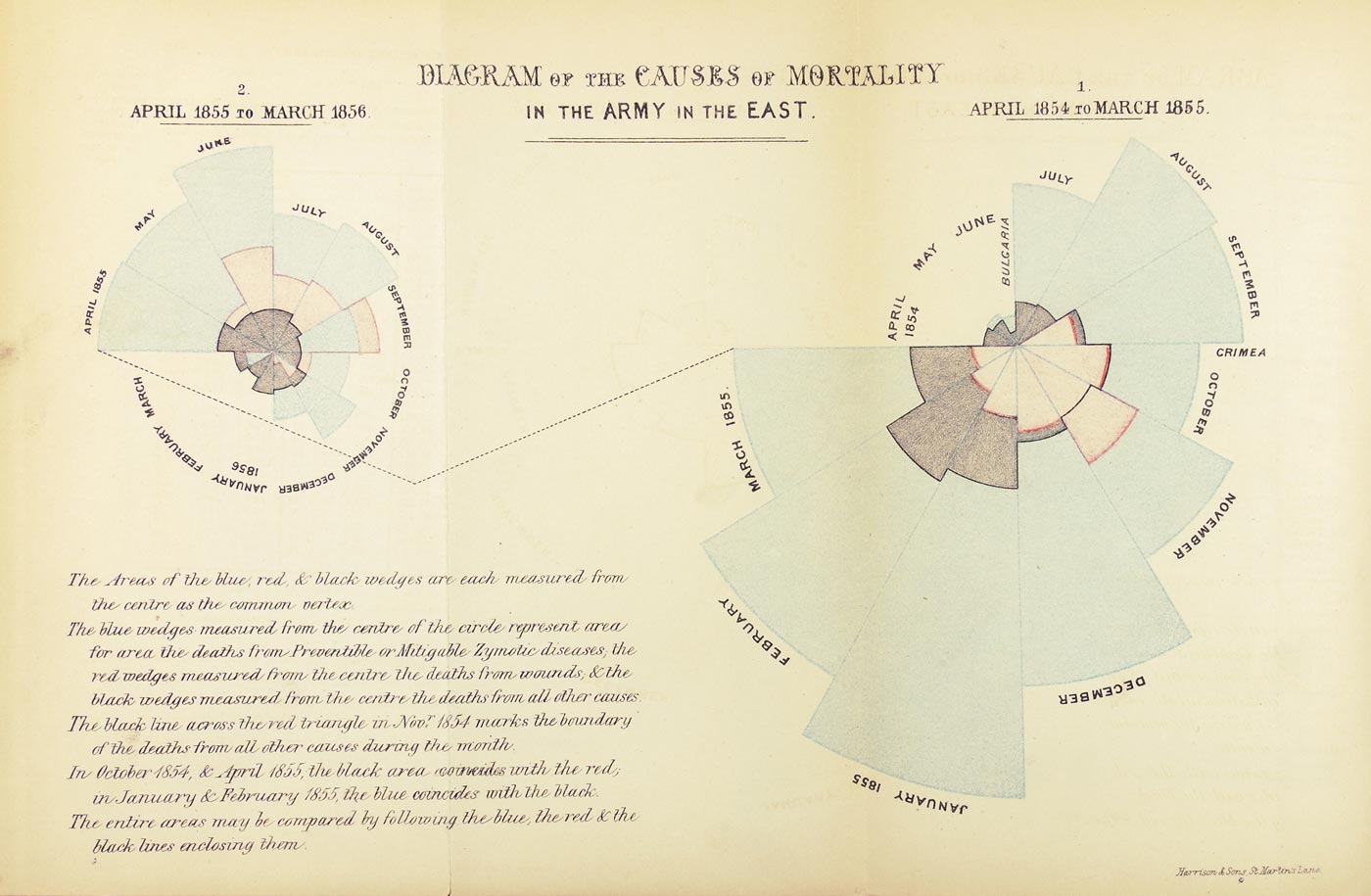
(Reproduced courtesy of the Florence Nightingale Museum) [View full size]
...she was ahead of her time in using evidence-based argument and what might be viewed today as infographics.Nightingale’s use of data to identify problems and visually convey their meaning is perhaps one of the many important gifts that she has given the profession. Her use of the polar area diagram, Figure 1, to convey the causes of death and the overwhelming numbers who died from preventable conditions attracted attention, engaged readers in exploring its meaning and left lasting impressions. Clearly, she was ahead of her time in using evidence-based argument and what might be viewed today as infographics. In short, the ability and power to visualize a situation should not be underestimated. Hence, if we are to maintain the progress she advocated, we also need to think about how to identify and communicate issues that impact populations and how, as nurses, we can address the opportunities for health improvement they present.
Synergizing Perspectives
Bibliometrics provides a means to synthesize the scholarly landscape...To bring together the two concepts identified in the quotes by Truman and Nightingale, we turn to a relatively new approach to examine the scholarly literature. Bibliometrics provides a means to synthesize the scholarly landscape and derive from the resulting analysis insights into the current and historical evolution of scholarship in the area of interest. Furthermore, through informed critique and consideration of the current policy landscape, future opportunities for contributions by nurses can be identified (Benton, Cusack, Jabbour, & Penney, 2017; Benton & Ferguson, 2017a). Accordingly, we seek to identify how nurses, relative to the medical profession, are contributing to scholarship on UHC and explore potential opportunities to leverage already-published work toward this agenda.
Method
This study used bibliometrics to analyze the published and peer-reviewed scholarship relating to UHC. As a means to assess the contribution of the nursing profession, we make a comparison with contributions of the medical profession. In addition, further bibliometric analysis is conducted in relation to nurse-led services as a means to explore how leading-edge practice may contribute to the attainment of UHC. As we contend, this is an opportunity for nurses around the world, irrespective of work setting, to make a difference to the health and well-being of all. As the study did not involve human subjects and the data is available to anyone with access to the Scopus database, no ethical approval was required.
The Role of Bibliometrics
Bibliometrics has its origins in the informational sciences but is increasingly used by nurses to examine diverse aspects of nursing scholarship. This can relate to the output of specific journals, institutions, or individuals (Benton & Alexander, 2016; Benton, 2017a). Also, it is used to track the evolution of scholarship in entire domains of interest or in more focused studies of interventions (Benton, Cusack, Jabbour, & Penney 2017; Benton, 2017b). In short, it is a flexible approach and can provide a wide range of metrics ranging from actual physical connections between authors to the identification of potential relationships between frequently occurring words in the titles and abstracts of papers (Yan and Ding, 2012).
In this article, a limited set of measures is used due to the ambitious scope of the analysis where three related, but different, data sets are examined: UHC both in relation to medicine and nursing, as well as nurse-led services. To that end, only those metrics used in the article will be elaborated. For those wishing a more comprehensive understanding of the potential usages of bibliometric analysis, there is a wide range of texts to consult (Cronin & Sugimoto, 2014; Gingras, 2016; TUDelft, 2017).
Data Source and Extraction
There are a variety of bibliographic databases that could be used to extract data for this study. However, in terms of medical and nursing scholarship coverage, the most comprehensive database of peer-reviewed content is found in Scopus (Elsevier) and accordingly is the database of choice (De Groote & Raszewski, 2012). To identify source material, standard keyword searching, along with the use of logical operators to narrow the search and the application of category delimiters (e.g., removing non-English articles), was used. Data was then extracted in comma-separated value files ready for uploading directly into the analysis software.
Data Analysis
VOSviewer uses multidimensional scaling to identify relationships between the variables of interest.Van Eck and Waltman (2010) conducted an analysis of a range of bibliographic analytical and visualization tools and concluded that VOSviewer was the most flexible and comprehensive. Since that time, there have been regular enhancements to the software package and, as a result, version 1.6.9 was used (Van Eck & Waltman, 2018). VOSviewer uses multidimensional scaling to identify relationships between the variables of interest. It then graphically represents these through visualization of similarities by placing those that are most closely related in near proximity. Those that have a more distant relationship are placed furthest apart.
As indicated earlier, there are a range of metrics that can be examined. For the purposes of this study, we limited the analysis to co-authorship, co-occurrence, and co-word analysis. The reason for selecting these three approaches related to our desire to examine how collaborative scholars are (co-authorship); the general dimensions addressed by the authors (co-occurrence); and as a means of identifying more detail within the various domains, the content of the scholarship currently addressed (co-word analysis). Each of these is briefly discussed below.
One way to look for the presence or absence of invisible colleges is to look at the co-authorship links relating to scholarship in a particular topic...Co-authorship Analysis. Diana Crane (1972) identified that scholars often create informal networks across institutions and beyond national country borders. She identified these as ‘invisible colleges’ and contended that the ability to mobilize advocacy in a coordinated manner across these networks can often make the difference between success and failure in influencing policy positions or completing research. One way to look for the presence or absence of invisible colleges is to look at the co-authorship links relating to scholarship in a particular topic where authors have contributed three or more times to the topic.
Co-occurrence Analysis. Co-occurrence analysis provides a means, through examination of the keywords used to describe the paper, to identify and describe underlying domains of scholarship contained within the corpus of publication being addressed by authors. This can help identify areas where there may be enough evidence to conduct further synthesis and thereby potentially strengthen the lines of argument that can be presented to policymakers.
Co-word Analysis. To obtain a more granular analysis of the content of scholarship, co-word analysis is used to identify patterns of commonly used terms within the titles and abstracts of the papers under review. This is particularly helpful when looking at topics where there is only a limited number of publications.
Results
The systematic search of Scopus resulted, after cleaning of data (i.e., removing non-English articles), in 2,471 UHC medical papers; 200 UHC nursing papers; and 1,495 nurse-led services papers. All subsequent analysis is based on the entirety of the content of these data sets.
There are a large number of unconnected authors who have, up to this point, contributed one or two papers each.Contrasting Medicine and Nursing
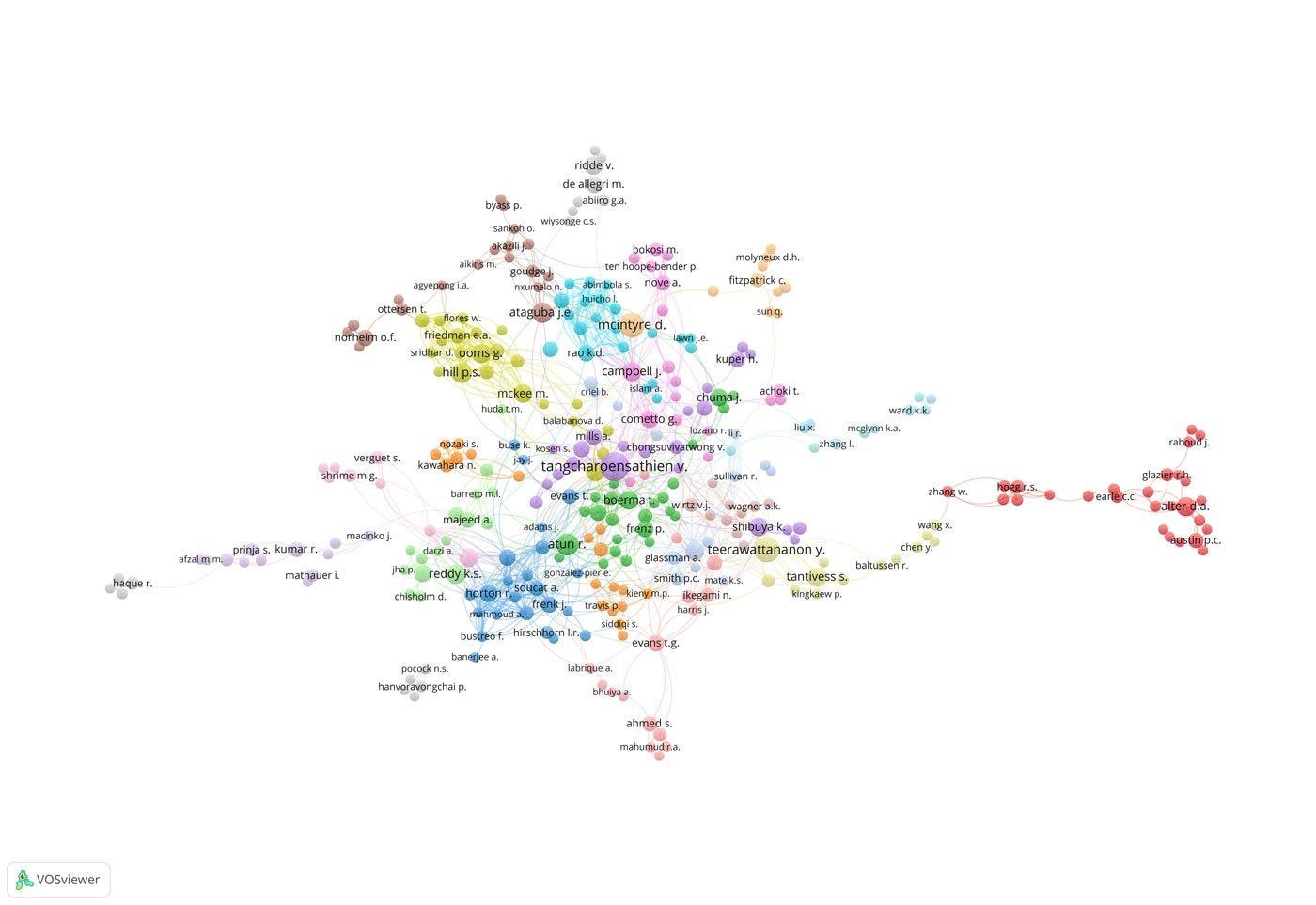
Co-authorship analysis of the UHC medicine data (Figure 2) demonstrates a well-developed network of invisible colleges. However, in the case of nursing, repeated contributions of three or more papers come from three individual authors and a single group of three collaborators. However, there is no connection between the three individuals and the small group. There are a large number of unconnected authors who have, up to this point, contributed one or two papers each.
Figure 2. Co-authorship Network Relating to Medical Articles on UHC
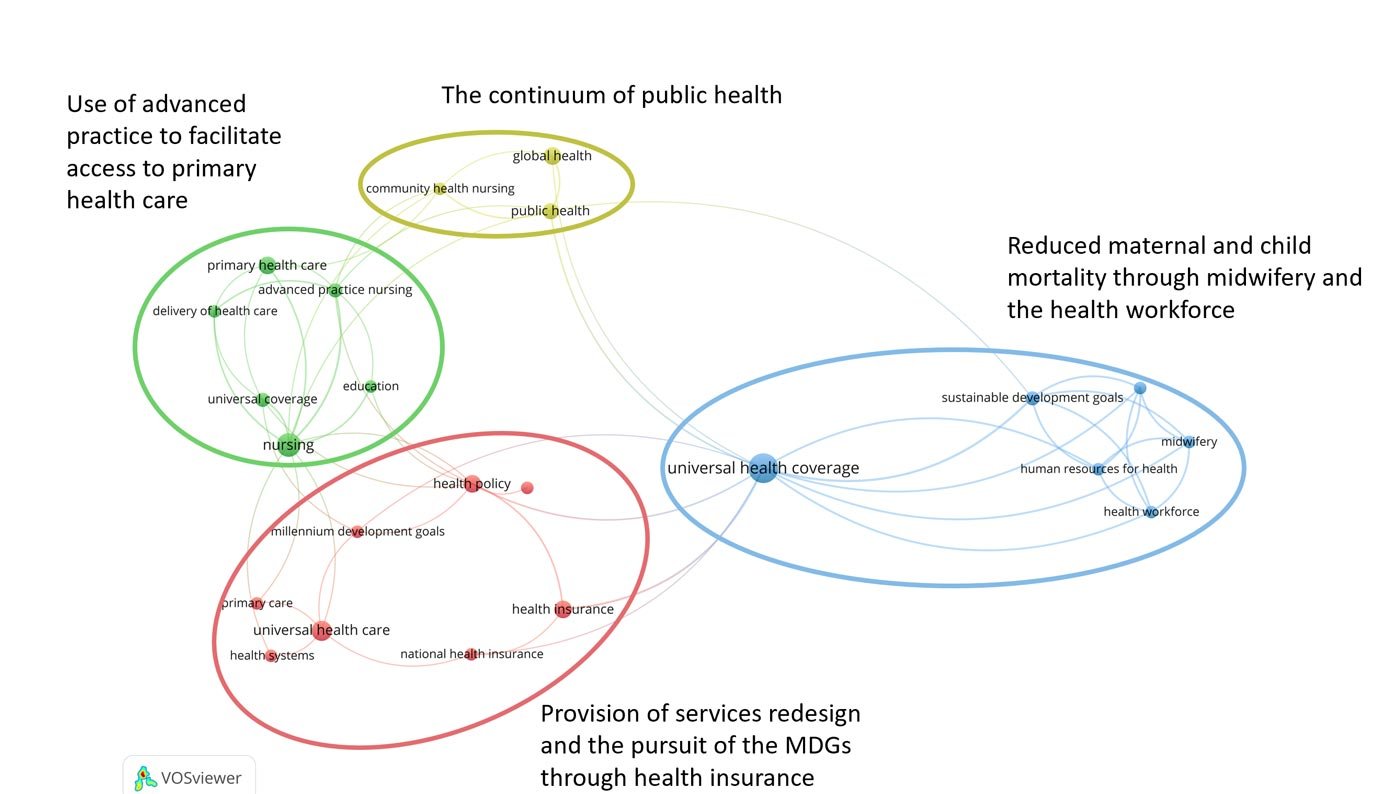
To look at the focus of this work, it is necessary to turn to co-occurrence analysis. By examining keywords used to classify the various papers, it is possible to identify underlying themes. Mapping data from the UHC nursing papers provides a very simple segmented visualization, as can be seen in Figure 3. There are four high-level clusters of terms that delineate material relating to: the provision of services redesign and the pursuit of the MDGs through health insurance; the use of advanced practice to facilitate access to primary healthcare; the linkage between attainment of reduced maternal and child mortality through midwifery and the health workforce; and the public health continuum from community to global health.
Figure 3 UHC Nursing Co-occurrence Analysis
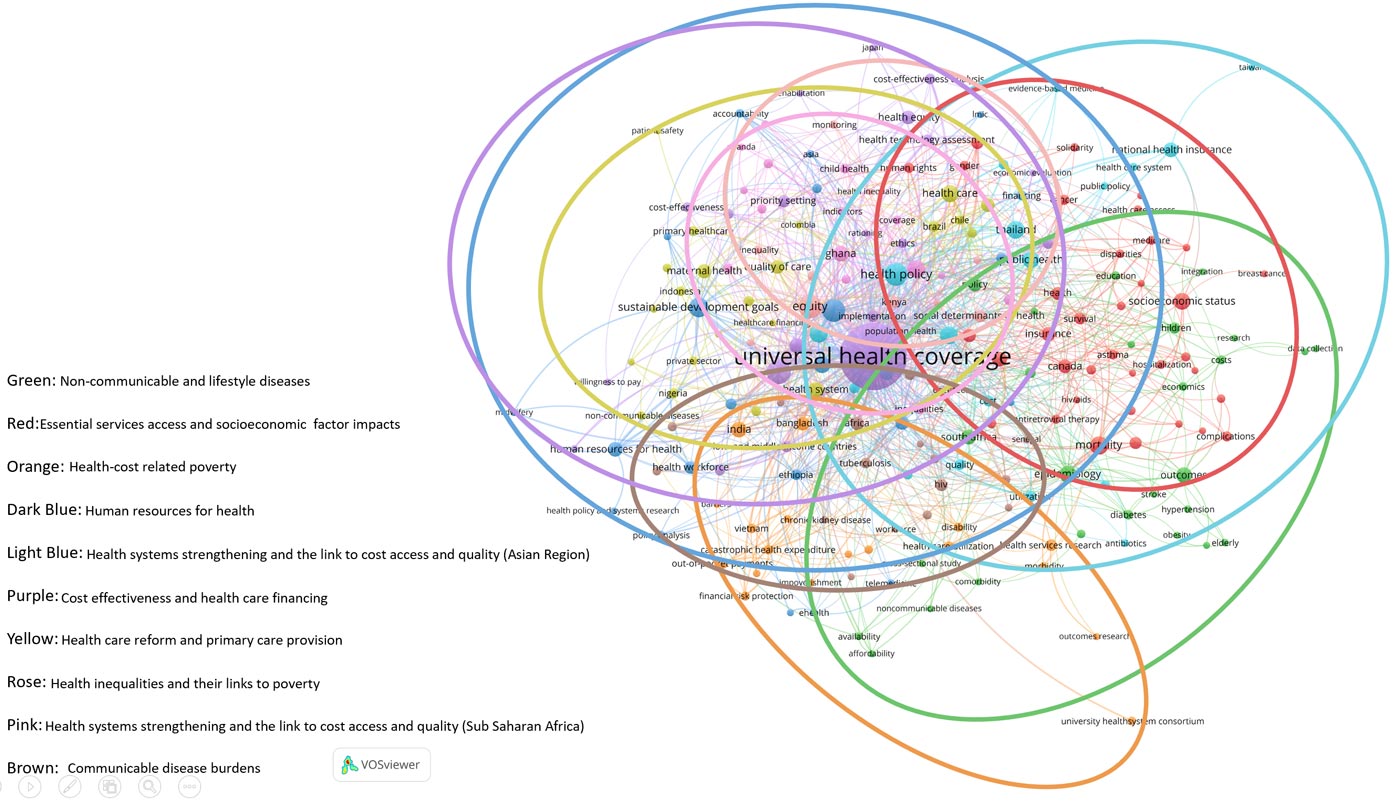
The situation relating to medicine is far more complex as can be seen from the 10 overlapping clusters of terms in Figure 4. These clusters relate to non-communicable and lifestyle diseases; essential services access and socioeconomic factor impacts; health cost-related poverty; human resources for health; health systems strengthening and the link to cost, access and quality in the Asian region; cost effectiveness and healthcare financing; healthcare reform and primary care provision; health inequalities and their links to poverty; health systems strengthening and the link to cost, access and quality in the sub-Saharan Africa region; and communicable disease burdens.
Figure 4 Medicine Co-occurrence Analysis
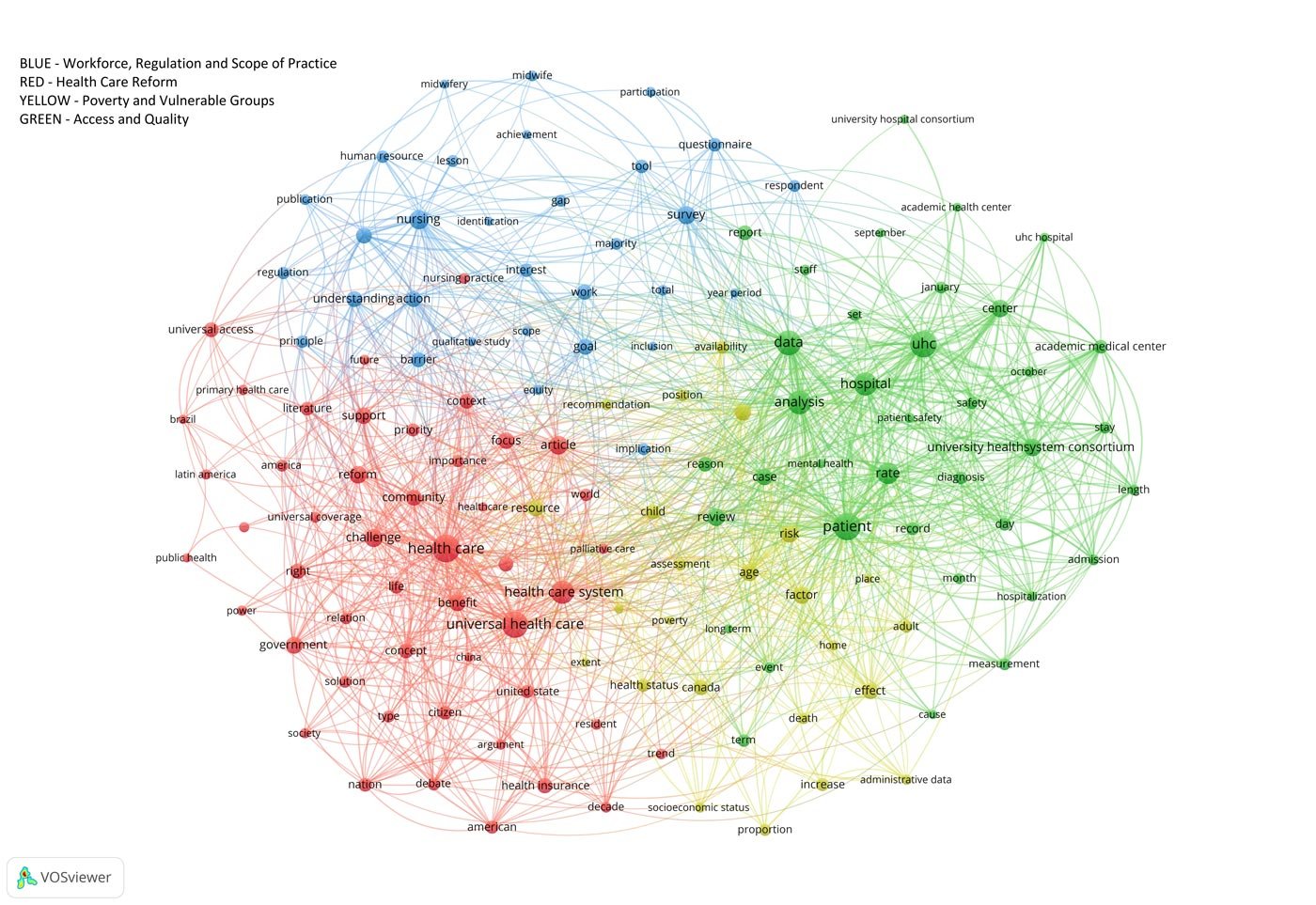
...nurse scholars are addressing the topic of UHC through a high-level general perspective...To gain deeper insight into the content of the publications, we conducted co-word analysis of the titles and abstracts. This, coupled with the co-occurrence analysis results, can help identify areas where there may be sufficient evidence to conduct a systematic review or meta-analysis. This potentially strengthens the lines of argument to present to policymakers. Unfortunately, Figure 5 confirms and elaborates slightly the findings identified in the co-occurrence analysis. That is, nurse scholars are addressing the topic of UHC through a high-level general perspective (e.g., healthcare reform; poverty and vulnerable groups; workforce, regulation and scope of practice; and access and quality). Hence, as will be seen later, an alternative approach is needed if nurses are to identify sufficient evidence to support evidence-based policy contributions to UHC.
Figure 5 Co-word Analysis of Nursing Titles and Abstracts from UHC Published Work
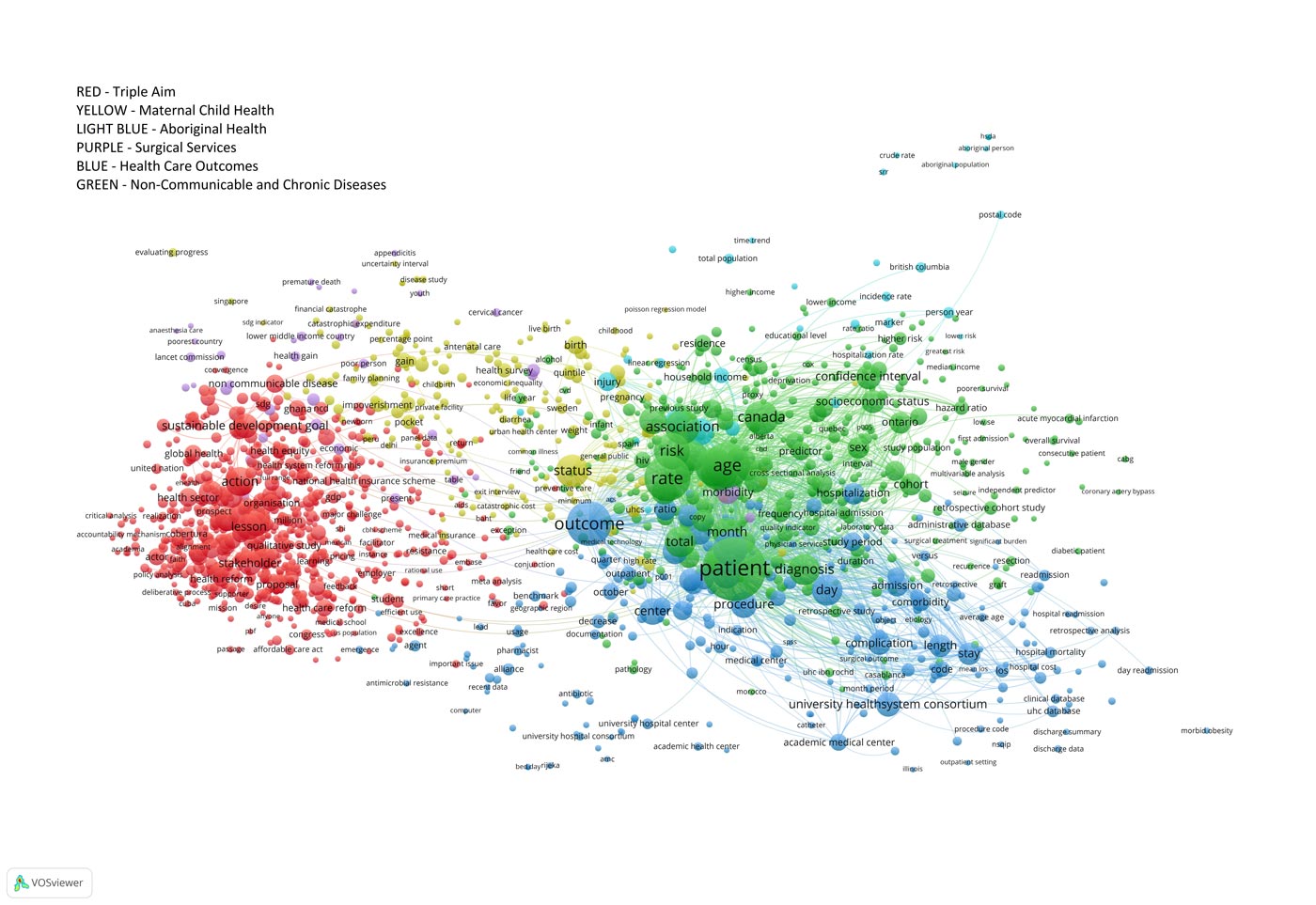
...medical scholarship is more clinically orientated, outcomes-focused, and comprehensive in addressing the balance between costs, access and quality of services.Examination of Figure 6, and contrasting the results of the co-word analysis of UHC medical literature with those identified from nursing, highlights that medical scholarship is more clinically orientated, outcomes-focused, and comprehensive in addressing the balance between costs, access and quality of services. The profession of nursing could learn from these differences and, if appropriate, collaborate with existing groups or initiate parallel nurse-focused programs of research. If we only look at UHC scholarship output, we see that the medical profession is currently in a stronger position to advocate for evidence-based change. This may be one reason why the medical profession tends to dominate the policy formulation landscape.
Figure 6 Co-word Analysis of Medical Titles and Abstracts from UHC Published Work
Leveraging Wider Nursing Scholarship
As indicated in the introduction, Crisp et al. (2018) highlighted a movement toward nurse-led services and this may provide a contribution to address provision of UHC. Indeed, authors such as Benton, Chapman, & Smith (2003) and Williamson et al. (2006) have already demonstrated the role that nurse-led services can play to increase access, reduce costs and improve quality. It is, therefore, logical to explore the literature on this topic to determine the potential to identify evidence that can be leveraged toward the UHC agenda. By examining some of the same metrics, it may be possible to provide concrete suggestions about how nursing scholarship can better contribute to the pursuit of UHC.
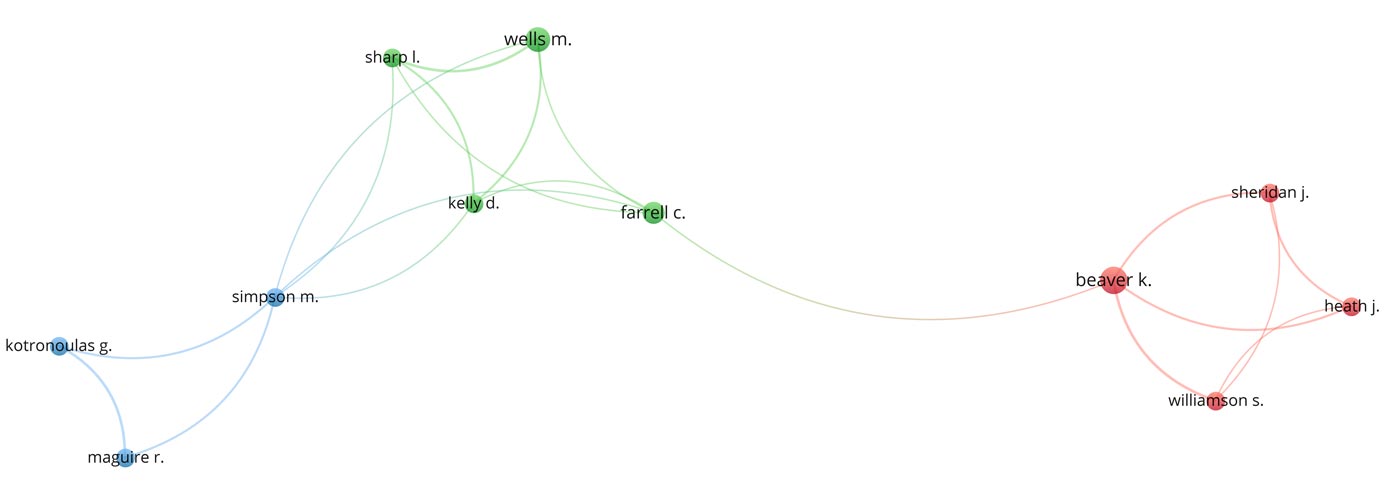
As was the case with UHC, where there is only limited collaboration between authors who have written three or more papers on the subject, co-authorship in nurse-led services was only marginally more connected than the UHC nursing landscape (Figure 7).
Figure 7 Co-authorship Network Relating to Nurse-led Services
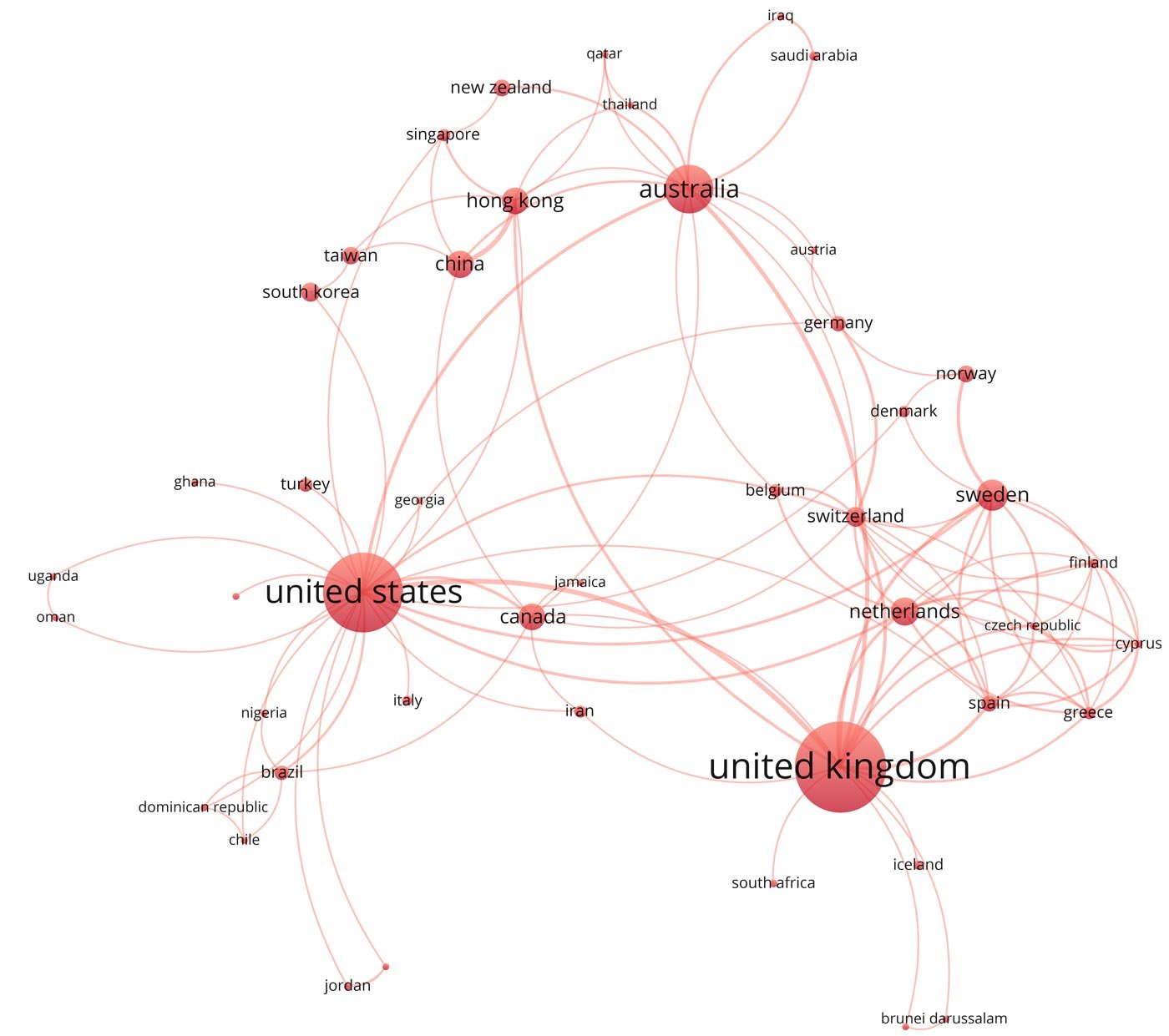
Another way to look at nurse-led services collaboration is to examine the authors’ countries of origin.Another way to look at nurse-led services collaboration is to examine the authors’ countries of origin. In this case, three countries are dominating scholarship, the United Kingdom, United States and Australia (Figure 8). Additionally, it is clear there is already a diverse range of low-, middle-, and high-income countries contributing to nurse-led services scholarship. As Figure 8 shows, it would appear that authors tend to collaborate in geographically proximal groups. This may well provide a target for increased local and regional collaboration, as well as opportunities to leverage local and regional connections among policymakers.
Figure 8 Co-authorship Network Relating to Nurse-led Services by Author Country of Origin
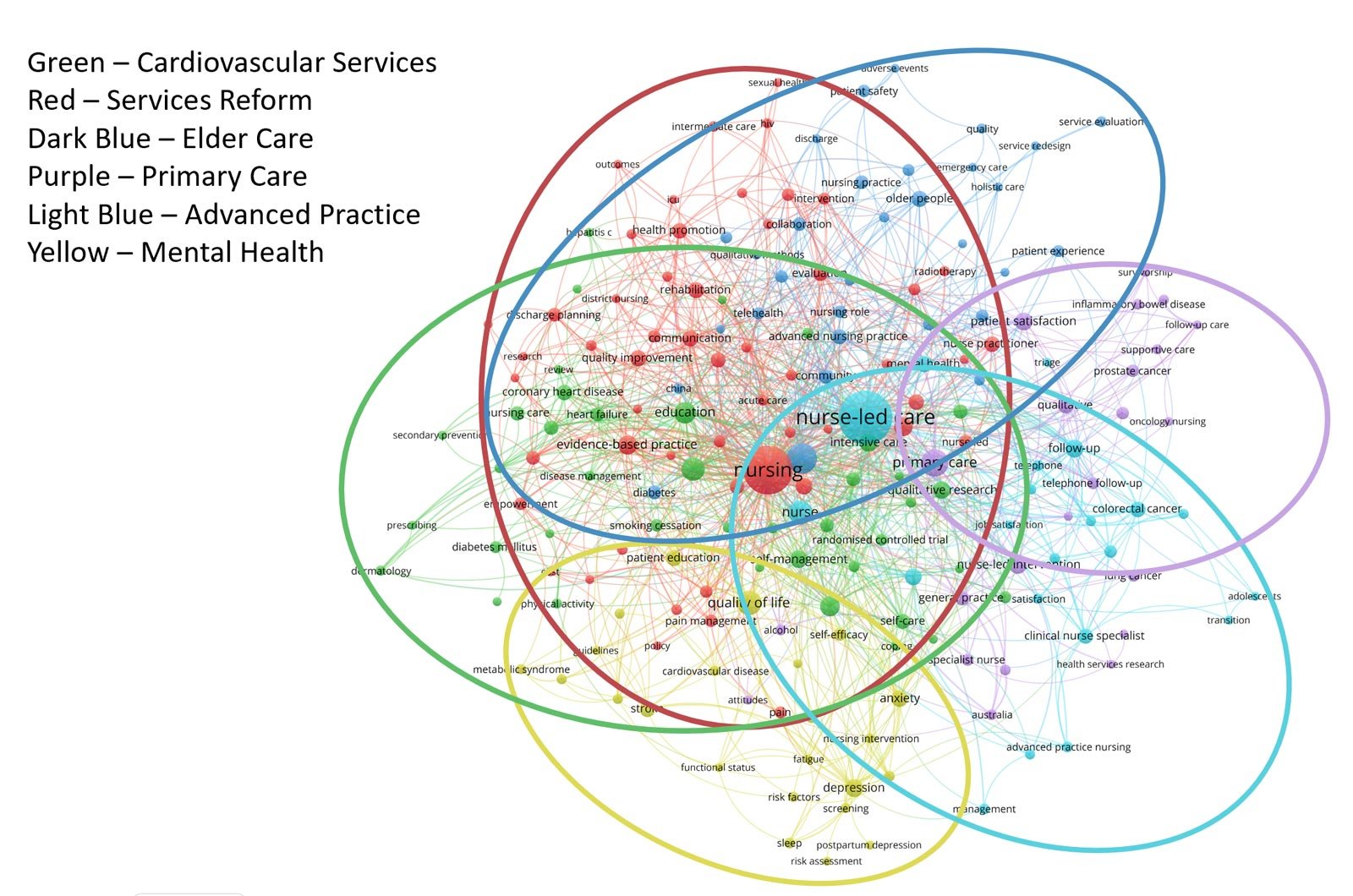
Co-occurrence analysis of the nurse-led care scholarship revealed six domains of inquiry focusing on cardiovascular services; service reform; elder care; primary care; mental health; and advanced practice roles (Figure 9). Several of these dimensions contained a significant quantum of publications that probably warrant further detailed inquiry via targeted integrative or systematic reviews. Such work may then provide more definitive guidance that could be more widely disseminated and implemented. Due to the client group orientation of some of this work it may be possible to engage other activist communities, such as user groups or condition-specific interest groups, to amplify any nursing messages.
Figure 9 Co-occurrence Analysis of Nurse-led Care Data Set
Discussion and Recommendations
Far too often the innovative work of nurses goes undocumented, unreported, and unacknowledged...Far too often the innovative work of nurses goes undocumented, unreported, and unacknowledged and as a result, makes the discovery of our history more difficult. Benton, Chapman, & Smith (2003) identified the wealth of innovation that takes place in a single health delivery system by nurses and, through systematically gathering evidence, was able to raise the profile of the profession within the system as well as provide a means to disseminate such practices more widely. Subsequently, Benton (2012) demonstrated that innovative practices by nurses were globally widespread across low-, middle-, and high-income countries. Yet nurses often do not report such efforts.
If nurses are to maximize their contributions, they need to document their endeavors in peer-reviewed journals. Such publications will facilitate discovery, provide assurance of scientific rigor and offer a mechanism to contribute to systematic reviews and meta-analysis, thereby informing policy choices. This analysis of the profession’s current contribution to UHC demonstrates that we have a way to go. But by reframing some of the existing work to address UHC, accelerated progress is possible. Increasingly, nurses are pursuing post-graduate degrees, so there is a growing quantum of scholarship available. Faculty and facility nurse leadership should encourage the publication of such work as part of a strategy toward raising the profession’s visibility and policy presence as well as a means of acknowledging contributions that individual and teams of nurses are making.
We could do this rapidly by leveraging existing work and reframing it in the form of policy briefs...Contributing to the Cost, Quality and Access Debate
As noted in the analysis of UHC evidence, nurses must examine and report on all three aspects of the cost-quality-access triangle (Benton, 1994). Each must be explored from multiple stakeholder perspectives. This may be possible though collaboration with economists and other members of the wider academic community. Nurses need to frame their work more broadly by highlighting their meta-policy-level contribution to UHC, SDGs, and other global initiatives, adding value, impact, and effect to the clinical improvements they can deliver.
By systematically curating and publishing the evidence, we can avoid duplicative efforts and maximize the application of nursing innovation, knowledge, and impact. We could do this rapidly by leveraging existing work and reframing it in the form of policy briefs rather than leaving it to languish in research journals (Wong, Bazemore, Green, & Miller, 2017). Although beyond the scope of this article, it would be possible through further bibliometric analysis of both systematic and meta-analytical studies to identify key content that could provide valuable material to take to the policy table.
The lack of any corpus of connected nursing authors is an important finding and represents a major opportunity.Invisible Colleges
From the co-authorship analysis of UHC data it is appropriate to conclude that the profession of medicine is more prolific and coordinated in its contributions. As Diana Crane (1972) noted, there exist a number of well-connected invisible colleges that collaborate and leverage their unique contributions for the furtherance of the discipline. The lack of any corpus of connected nursing authors is an important finding and represents a major opportunity. By establishing networks of colleagues there is potential to generate synergy across areas of inquiry that will better position the profession to influence individual governments and global policy.
It is perhaps not surprising that networks of UHC research collaboration do not exist. The lack of networks across nursing leadership, especially at the global level, is well documented (Benton & Ferguson, 2014; 2016). The same authors also demonstrated that with modest input via e-mail, networks could, once established, be maintained relatively easily (Benton & Ferguson, 2017b). These networks could provide the platform for coordinated advocacy. Furthermore, this analysis demonstrates that nurses are pursuing a number of emergent areas of research on UHC and this may be an opportunity for nurse academics and/or the WHO Nursing Collaborating Centers to develop these into full programs of research and policy action.
Only by documenting nurses’ work can their impact on health outcomes be properly examined.Comprehensive Workforce Strategy
Unfortunately, the work of nurses is almost invisible due to their lack of inclusion within the electronic health record (Moody, Slocumb, Berg, & Jackson, 2004). Nursing care is frequently costed as part of room and board. Since nursing is the largest of all the health professions, and in some cases nurses can deliver up to 80% of care, lack of documentation of nursing interventions and consequent impacts on patient outcomes makes any workforce strategy at best imprecise, and at worst meaningless. Only by documenting nurses’ work can their impact on health outcomes be properly examined. Only when such data is available will it be possible to undertake correlation studies to inform decisions about team composition through the optimization of costs, access, and quality by actively considering the effective and efficient contribution of various team members.
Supportive Legislation and Regulation
The literature did highlight that some of the work, both in the UHC and the nurse-led services space, is examining issues of scope of practice. This is a critical component of health systems redesign. Regulation that was developed for the industrial era must be replaced by regulatory processes that are fit for today’s complex, global, and digital world (Benton, 2017b). Recent developments such as the NCSBN Regulatory Atlas (Global Regulatory Atlas, n.d.) provide information on 319 jurisdictions encompassing 20.5 plus million nurses from around the globe. This database is expanded on a weekly basis and the figures are correct as of March 7, 2019. The atlas offers a way for jurisdictions to compare and contrast their approach with those of other countries. Use of such tools provides a means of reaching out to peers and, through dialogue, gain insights on ways to reform regulation and legislation.
To be effective, nurses must engage at all policy levels and avoid a sole focus on high-level dialogue.Profile and Status
Often nurses become fixated on representation at the highest policymaking tables (Juma, Edwards, & Spitzer, 2014; Nagle, 2014; Polansky, Gorski, Green, Perez, & Wise, 2017). This is important, but only part of what needs to be done if the nursing voice is to be heard and its profile and status raised. To be effective, nurses must engage at all policy levels and avoid a sole focus on high-level dialogue. To this end, Brownson, Chriqui, & Stamatakis (2009) suggested a need to better understand barriers and levers for engaging and bringing about policy change. Recent work by Woodward, Smart, and Benavides-Vaello (2016) identified that one way to address this is to target modifiable factors that support the contribution of nurses to policy and politics.
Three modifiable factors were identified: integration of political education in the nursing curriculum; the value of active psychological engagement; and the value of collective influence. Furthermore, Benton and Shaffer (2016) have suggested that by equipping nurses with the necessary skills, the profession of nursing has a wide range of contributions to make across all 17 of the sustainable development goals. Sometimes this can be accomplished through action, sometimes through advocacy, and sometimes through the alignment of the profession with others. To do this, Benton, Al Maaitah, & Gharaibeh (2017) highlighted a need to clearly set out policy and political competencies needed by nurses at all levels and not simply promote it as an opportunity to lobby government.
Ellenbecker et al. (2017) made a partial attempt to address this in a publication about a staged approach to educate nurses in health policy. However, while their proposals are a welcome addition, they cluster Doctor of Nursing Practice (DNP) and Doctor of Philosophy (PhD) competencies together; draw upon U.S. nursing literature, and fail to explore work undertaken in the wider policy space. The work of Ellenbecker et al. (2017) needs further exploration to differentiate between DNP and PhD roles, as well as include policy competencies for both the sub-baccalaureate level and diploma-prepared individuals. It is only when nurses contribute in such a wide manner, at all levels, that the potential of the nursing profession will be optimized, its voice heard, its profile raised, and its contribution valued.
Promoting Existing Resources
This study has identified several opportunities for nurses to contribute to the UHC policy landscape. To assist in pursuing such opportunities, there are a great deal of freely accessible resources to help nurses develop policy advocacy skills. Some are highly focused and address a single dimension of raising a policy voice and the visibility of the profession, such as guides to writing for scholarly publication or writing policy briefs (Wiley, 2014; Young & Quinn, 2017). Other material is far more comprehensive and provides what can best be described as a series of distance learning modules or a toolkit that offers a relatively comprehensive grounding in various aspects of contributions to health policy (WHO Western Pacific Region, 2005). Nursing Now! could curate such resources and include them on its website, providing a focused, high-quality suite of documents to share with partners and nursing groups affiliated with the campaign.
We do not need to reinvent the wheel, but we do need to disseminate knowledge more effectively and efficiently as our scholarship and networks grow.Exploiting Growing Capacity
Florence Nightingale was well-educated, well-connected, and grounded in the realities of practice. She was also passionate about finding solutions to the problems she identified. As more and more nurses attain higher levels of education, the capacity to emulate Nightingale’s work and those that followed in her footsteps is enhanced. To this point, nursing as a profession has not been as prolific in the scholarship space as has medicine. The findings of this study serve as a benchmark to measure progress. As a result of this study, we can now look at creation of invisible colleges and development of themes as we address topics relevant to the SDGs in general, and UHC in particular. Most importantly, we can leverage some existing work toward the UHC agenda. We do not need to reinvent the wheel, but we do need to disseminate knowledge more effectively and efficiently as our scholarship and networks grow. That is the challenge we face as we enter the bicentennial of Nightingale’s legacy. By looking at successes of other nurse luminaries from around the world, we can, as Nightingale posited, keep moving forward, building upon lessons learned, and tackling opportunities identified.
A Global Social Movement and Recommendations to Advance It
One objective of Nursing Now! is to develop a global social movement. By looking at co-authorship from the perspective of the countries from which authors originate and are connected, it is possible to identify and leverage existing networks. We believe that digital platform links, once made, can be maintained (Benton & Ferguson, 2017b). We note that nurses tend to develop proximal geographic links, but with the advent of social media as a tool in knowledge transfer, wider and more rapid dissemination is possible (Reed, 2018). Accordingly, we recommend that existing professional societies, associations, and regional structures (e.g., the WHO regional offices) capitalize on this when seeking to obtain policy input at national, regional, and global levels.
One objective of Nursing Now! is to develop a global social movement.Entities such as the WHO Nursing Collaborating Centers should initiate and promote publication of policy briefs as parallel documents to systematic and meta-analytical studies. As a starting point, a bibliometric analysis of such studies should be conducted to identify areas that will make an optimal nursing contribution to the pursuit of UHC and help address other relevant SDGs. Furthermore, journals should mirror the efforts of the International Nursing Review to highlight policy implications of published scholarship. Such efforts, we believe, will provide a rich source of material for use in local, national, regional, and international advocacy efforts.
Recent work (Benton, Al Maaitah, & Gharaibeh, 2017; Ellenbecker et al., 2017; Woodward et al. 2016) has identified the need for increased education in political participation and policy analysis. We recommend further work to expand and elaborate the competencies proposed by Ellenbecker et al. (2017) to equip nurses with the necessary knowledge, skills, and behaviors to effectively contribute to and influence policy at all levels.
Limitations
Due to software limitations, we were unable to analyze material published in any language other than English. However, this resulted in the rejection of less than 2% of the papers. Examination of the titles suggests that these papers were replicative in terms of material. Therefore, we believe that this limitation had minimal impact on our findings.
Conclusion
We set out to examine how nurses contribute to UHC scholarship and compare it with the contributions of the medical profession. In the process, we have identified that the profession of nursing lags significantly behind the medical profession, but can potentially make rapid progress if the isolated efforts of researchers are harnessed and the existing work on nurse-led services is applied to the pursuit of UHC. We have established a baseline of current nursing scholarship that can be used to assess progress. And, we have offered concrete suggestions for further work.
In pursuing our focus on UHC, we have also addressed other dimensions of the Nursing Now! objectives. Specifically, we have identified opportunities to increase and improve the dissemination of effective and innovative practice in nursing; examine the medical contribution to UHC for opportunities for collaboration and/or the pursuit of original work; and propose leveraging existing work and adding value by curating the evidence and through the production of policy briefs to inform change.
If the profession of nursing can harness the full potential of its enormous global workforce...then the possibilities for change are limitless.If the profession of nursing can harness the full potential of its enormous global workforce through energizing and engaging staff at all levels in policy processes, then the possibilities for change are limitless. The impact on access, quality, and cost would be truly profound, and would be a fitting tribute to the work of Nightingale and so many other outstanding nurses that have contributed to our profession over the years. In reality, it is not just Nightingale that we should celebrate but instead use the bicentennial as a focus for all nurses who contributed to the advancement of our profession.
If Nursing Now! can bring about the planned global social movement, then the 200th anniversary of Nightingale’s birth in 2020 could form the basis of a paradigm shift for the profession. More importantly, imagine the impact on the health of nations and the attainment of UHC that such a change would bring. As Truman reminded us, familiarity with history can provide us with insights into the challenges we face. We believe that this bibliometric analysis has provided lessons that position the nursing profession to pick up the mantel vacated by our predecessors. It is now up to us to continue to march forward.
Authors
David C. Benton, PhD, RN, FRCN, FAAN
Email: dbenton@ncsbn.org
Dr. Benton hails from the North East of Scotland. He completed his RN education at Highland College of Nursing and Midwifery in Inverness, specializing in both general and mental health practice. He undertook his MPhil degree studying the application of computer assisted learning to post basic psychiatric nurse education at the University of Abertay and received a PhD Summa Cum Laude from the University of Complutence Spain, for his groundbreaking work on an international comparison of nursing legislation. Prior to his current post as Chief Executive Officer of the National Council of State Boards of Nursing, he worked for ten years at the International Council of Nurses based in Geneva, Switzerland. Benton is a prolific author and has published over 200 papers on leadership, workforce, health policy, social network analysis, bibliometrics, and regulation. He is a global expert in regulation and health and nursing policy and has advised governments around the world about both nursing legislation and wider health policy issues.
Christine J. Beasley, DBE, RN
Email: christine.beasley@icloud.com
Beasley began training in 1962 at the Royal London Hospital and worked as a staff nurse. In the 1980s/early 90s, she held senior roles at the Ealing and Riverside Health Authorities, before moving into wider regional nurse director posts at North Thames Regional Health Authority.
She has held a range of senior posts with a broad experience of policy development, leadership, and general management, including Head of Development with the Directorate of Health and Social Care, and Director of Nursing, Human Resources, and Organizational Development with the NHS Executive. She established the London Standing Conference, engaging nurses across the capital in leading service improvement and contributing to improvements in clinical practice across the country. Beasley was appointed as Chief Nursing Officer for England in October 2004 and is the Director within the Department of Health with the lead for Patient and Public involvement, the Allied Health Professionals and Healthcare Scientists, and was also the lead director for the voluntary and community sector. Since retirement she has held a number of non-executive appointments, including chair of the Florence Nightingale Museum Trust and a Trustee of the Burdett Trust for Nursing.
Stephanie L. Ferguson, PhD, RN, FAAN, FNAP
Email: drsferguson@stanford.edu
Dr. Ferguson is a global healthcare consultant with more than 35 years of experience designing, implementing, and evaluating health-related strategic plans and programs. As founder of Stephanie L. Ferguson & Associates, LLC, she has worked in 100+ nations as a technical advisor, consultant, and facilitator for the World Health Organization (WHO) and the International Council of Nurses (ICN). For WHO, she develops initiatives to strengthen and evaluate global healthcare delivery, population health outcomes, and health professional education and services. At ICN, she directed the Leadership for Change Programä and the ICN-Burdett Global Nursing Leadership Instituteä in Geneva, Switzerland. Dr. Ferguson was a White House Fellow from 1996-97 and is president-elect of the Foundation’s Alumni Association. She serves on the Bon Secours Mercy Health System board and its Strategy and Finance Committee. She is an elected member of the American Academy of Nursing; the National Academy of Medicine, where she serves on its Nominating Committee; and, the National Academies of Practice. Current faculty appointments include Consulting Associate Professor, Bing Stanford in Washington Program; and, Professor at the University of Lynchburg College of Health Sciences. She holds a PhD from the University of Virginia (UVA), a Master’s degree from the Virginia Commonwealth University, and a BSN from UVA.
References
Benton, D .C. (1994). The NHS market: NHS counter culture. Nursing Standard, 8(19), 48-50. doi: 10.7748/ns.8.19.48.s59
Benton, D. C. (2012). Advocating globally to shape policy and strengthen nursing’s influence OJIN: The Online Journal of Issues in Nursing, 17(1), Manuscript 5. doi: 10.3912/OJIN.Vol17No01Man05
Benton, D. C. (2017a). Using bibliometrics to support revalidation requirements. Nursing Standard, 32(1), 44-51. doi: 10.7748/ns.2017.e10589
Benton, D. C. (2017b). Bibliometric review: Identifying evolving and emergent regulatory trends. In Regulation 2030 First Steps on a Journey. Journal of Nursing Regulation, 8(2), S5-S14. doi: 10.1016/S2155-8256(17)30125-4
Benton, D. C., & Alexander, M. (2016). The Journal of Nursing Regulation at age 6: A bibliographic analysis. Journal of Nursing Regulation, 7(2), 4-8. doi:10.1016/S2155-8256(16)31072-9
Benton, D. C., Al Maaitah, R., & Gharaibeh, M. (2017). An integrative review of pursuing policy and political competence. International Nursing Review, 64(1), 135-145. doi: 10.1111/inr.12275
Benton, D. C., Chapman, C., & Smith, E. (2003). Sharing experience and learning. Nursing Management, 10(8), 24-27. http://dx.doi.org/10.7748/nm2003.12.10.8.24.c1957
Benton, D. C., Cusack, L., Jabbour, R., & Penney, C. (2017). A bibliographic exploration of nursing’s scope of practice. International Nursing Review, 64(2), 224-232. doi: 10.1111/inr.12337
Benton, D. C., & Ferguson, S. L. (2014). How nurse leaders are connected internationally: An exploratory study. Nursing Standard. 29(16), 44-48. doi: 10.7748/ns.29.16.42.e9060
Benton, D. C., & Ferguson, S. L. (2016). How anxiety about communication affects the role of nurse leaders in international social networks. Nursing Management, 23(2), 30-37. doi: 10.7748/nm.23.2.30.s27
Benton, D. C., & Ferguson, S. L. (2017a). Opportunities for change: The United Nations working for health and growth report. Nursing Management, 24(5), 26-30. doi: 10.7748/nm.2017.e1604
Benton, D. C., & Ferguson, S. L. (2017b). Sustaining a global social network: A quasi-experimental study. International Nursing Review, 64(1), 42-49. doi: 10.1111/inr.12270
Benton, D. C., Pérez-Raya, F., Fernandez-Fernandez, M. P., & González-Jurado, M. A. (2015). A systematic review of nurse-related social network analysis studies. http://dx.doi.org/10.1111/inr.12161
Benton, D. C., & Shaffer, F. (2016). How the nursing profession can contribute to the Sustainable Development Goals. Nursing Management, 23(7), 29-34. doi: 10.7748/nm.2016.e1534
Brownson, R. C., Chriqui, J.F., & Stamatakis, K.A. (2009). Understanding evidence-based public health policy. American Journal of Public Health, 99(9), 1576-1583. doi: 10.2105/AJPH.2008.156224
Burdett Trust for Nursing. (n.d.). Nursing Now. Retrieved from https://www.btfn.org.uk/nursing-now/
Crane, D. (1972). Invisible colleges: Diffusion of knowledge in scientific communities. Chicago, IL: University of Chicago Press.
Cronin, B., & Sugimoto, C.R. (2014). Beyond bibliometrics: Harnessing multidimensional indicators of scholarly impact. Cambridge, MA: Massachusetts Institute of Technology.
Crisp, N., Brownie, S., & Refsum, C. (2018). Nursing and midwifery: The key to the rapid and cost-effective expansion of high-quality universal health coverage. Retrieved from the World Innovation Summit for Health website: http://www.wish.org.qa/wp-content/uploads/2018/11/IMPJ6078-WISH-2018-Nursing-181026.pdf
De Groote, S. L., & Raszewski, R. (2012). Coverage of Google Scholar, Scopus and Web of Science: A case study of the h-index in nursing. Nursing Outlook, 60(6), 391–400. doi: 10.1016/j.outlook.2012.04.007
Ellenbecker, C. H., Fawcett, J., Jones, E. J., Mahoney, D., Rowlands, B., & Waddell, A. (2017). A staged approach to educating nurses in health policy. Policy, Politics and Nursing Practice, 18(1), 44-56. doi: 10.1177/1527154417709254
Gingras, Y. (2016). Bibliometrics and research evaluation: Uses and abuses. Cambridge, MA: MIT Press.
Global Regulatory Atlas. (n.d.). NCSBN Global Regulatory Atlas. Retrieved from https://regulatoryatlas.com/
International Council of Nurses. (n.d.). Nursing Now. Retrieved from https://www.icn.ch/what-we-do/campaigns/nursing-now
Juma, P. A., Edwards, N., & Spitzer, D. (2014). Kenyan nurses involvement in national policy development processes. Nursing Research and Practice, 2014, 1-10. doi: 10.1155/2014/236573
Miller, M. (1974). Plain Speaking: An oral biography of Harry S. Truman. New York, NY: Tess Press.
Moody, L. E., Slocumb, E., Berg, B., & Jackson, D. (2004). Electronic health records documentation in nursing: Nurses’ perceptions, attitudes, and preferences. Computers Informatics Nursing, 22(6), 337-344.
Nagle, L. (2014). An interview with Dr. Judith Shamian President, International Council of Nurses. Nursing Leadership, 27(1), 26-30.
Nash, R. (1914). Florence Nightingale to her nurses: A selection from Miss Nightingale’s addresses to probationers and nurses of the Nightingale School at St. Thomas’s hospital. London, England: Macmillan and Co., Limited.
Nicholson, D., Yates, R., Warburton, W., & Fontana, G. (2015). Delivering universal health coverage: A guide for policy makers. Retrieved from the World Innovation Summit for Heath website: http://www.wish.org.qa/wp-content/uploads/2018/01/WISH_UHC_Forum_Report_08.01.15_WEB.pdf
Nightingale, F. (1859). A contribution to the sanitary history of the British army during the late war with Russia. London, England: John W. Parker and Son.
Oxman, A. D., Lavis, J. M., & Fretheim, A. (2007). Use of evidence in WHO recommendations. The Lancet, 369(9576), 1883-1889. doi: 10.1016/S0140-6736(07)60675-8
Polansky, P., Gorski, M. S., Green, A., Perez, G. A., & Wise, R. P. (2017). Nurses leading change to advance health. Nursing Outlook, 65(6), 746-752. doi: 10.1016/j.outlook.2017.04.004
Reed, M. S. (2018). The research impact handbook (2nd ed.). Huntly, Scotland: Fast Track Impact Ltd.
River, C. (2018). Florence Nightingale: The life and legacy of the most famous nurse in history. Lexington, KY: Charles River Editors.
Small, H. (2017). A brief history of Florence Nightingale and her real legacy, a revolution in public health. London, England: Robinson.
TUDelft. (2017). Research positioning and trend identification [Booklet]. The Hague, Netherlands: Delft University of Technology. Retrieved from http://aida.tudelft.nl/toolbox/aida-booklet
United Nations. (2015). Transforming our world: The 2030 agenda for sustainable development [PDF file]. Retrieved from https://sustainabledevelopment.un.org/content/documents/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf
Van Eck, N. J., & Waltman, L. (2010). Software survey: VOSviewer. A computer program for bibliometric mapping. Scientometrics. 84(2), 523-538. doi: 10.1007/s11192-009-0146-3
Van Eck, N. J., & Waltman, L. (2018). VOSviewer manual [PDF file]. Leiden, The Netherlands. University of Leiden. http://www.vosviewer.com/documentation/Manual_VOSviewer_1.5.4.pdf
Wiley. (2014). Writing for publication: An easy to follow guide for nurses wanting to publish their work [PDF file]. Oxford, England: John Wiley and Sons, Inc. Retrieved from http://www.wiley-docs.com/HSJ-14-63694_Writing_for_Publication_lowres.pdf
Williamson, T., Rawle, A., Bacon, E., Cooper, E., Eastwood, J., Evans, A.,…Whitworth, J. (2006). An evaluation of a nurse-led unit: An action research study. Manchester, England: University of Salford/Derbyshire County PCT. http://usir.salford.ac.uk/12868/1/PDF_Nurse_Led_Evaluation_FINAL_REPORT_05.02.07.pdf
Wong, S. L., Bazemore, A. W., Green, L. A., & Miller, B. F. (2017). How to write a health policy brief. Families, Systems and Health, 35(1), 21-24. doi: 10.1037/fsh0000238
Woodward, B., Smart, D. & Benavides-Vaello, S. (2016). Modifiable factors that support political participation by nurses. Journal of Professional Nursing, 32(1), 54-61. doi: 10.1016/j.profnurs.2015.06.005
The World Bank. (n.d.). Universal health coverage. Retrieved from https://www.worldbank.org/en/topic/universalhealthcoverage
World Health Organization. (n.d.a). Nursing Now. Retrieved from https://www.nursingnow.org/
World Health Organization. (n.d.b). Nursing Now campaign. Retrieved from https://www.who.int/hrh/news/2018/nursing_now_campaign/en/
World Health Organization Western Pacific Region. (2005). Health service planning and policy-making: A toolkit for nurses and midwives. Geneva, World Health Organization. http://apps.who.int/iris/handle/10665/207061
World Health Organization, World Bank Group, Organization of Economic Cooperation and Development. (2018). Delivering quality health services: A global imperative for universal health coverage. Geneva, Switzerland: World Health Organization. Retrieved from http://apps.who.int/iris/bitstream/handle/10665/272465/9789241513906-eng.pdf?ua=1
Yan, E. & Ding, Y. (2012). Scholarly network similarities: How bibliographic coupling networks, citation networks, co-citation networks, topical networks, co-authorship networks and co-word networks relate to each other. Journal of the American Society for Information Science and Technology, 63(7), 1313-1326. doi: 10.1002/asi.22680
Young, E. & Quinn, L. (2017). An essential guide to writing policy briefs [PDF file]. Berlin, Germany: International Centre for Policy Advocacy. Retrieved from http://www.icpolicyadvocacy.org/sites/icpa/files/downloads/icpa_policy_briefs_essential_guide.pdf