


Keeping patients safe is a core nursing duty. The dynamic nature of the healthcare environment requires that nurses practice to the full extent of their education, experience, and role to keep patients safe. Research has focused on error causation rather than error recovery, a process that occurs before patient harm ensues. In addition, little is known about the role nurses play in error recovery. A descriptive cross-sectional, correlational study using a sample of 184 nurses examined relationships between nurse characteristics, organizational factors, and recovery of medical errors among medical-surgical nurses in hospitals. In this article, we provide background information to introduce the concept of error recovery, and present our study aims and methods. Study results suggested that medical-surgical nurses recovered on average 22 medical errors and error recovery was positively associated with education and expertise. The discussion section further considers the important role of medical-surgical nurses and error recovery to enhance patient safety. In conclusion, we suggest that creating a safer healthcare system will depend on the ability of nurses to fully use their education, expertise and role to identify, interrupt, and correct medical errors; thereby, preventing patient harm.
Key Words: Patient safety, medical error, errors, medical-surgical, nurses, error recovery, expertise, certification, workload, scope of practice, educational level
Since the focus on error prevention has not yielded expected results to make healthcare safer, it is reasonable to explore the notion of error recovery. Making healthcare safer is a national mandate, yet little progress has been made to reduce the medical error rate in the past 15 years (Aranaz-Andrés et al., 2011; Landrigan et al., 2010). Since the focus on error prevention has not yielded expected results to make healthcare safer, it is reasonable to explore the notion of error recovery (Gaffney, Hatcher, & Milligan, 2016). Errors are actions that fail to meet their desired outcome (Institute of Medicine, 2000). The recovery process consists of identifying, interrupting, and correcting medical errors to mitigate patient harm. Safety conscious organizations must anticipate that errors will occur and incorporate error recovery strategies into patient safety efforts (Habraken & van der Schaaf, 2010; Helmreich, 2000; Reason, 1990).
The dynamic nature of the healthcare environment requires that nurses practice to the full extent of their education, experience, and role in order to keep patients safe. Patient safety is a core nursing duty. The dynamic nature of the healthcare environment requires that nurses practice to the full extent of their education, experience, and role in order to keep patients safe (American Nurses Association, 2015). Although nurses play a key role in safeguarding patients, little is known about their role in recovering medical errors. Further examination of nurses’ role in the recovery process can provide important insight into positive recovery factors and the optimal utilization of registered nurses (RNs) in order to enhance patient safety.
In this article, we will provide background information to introduce the concept of error recovery, and present our study aims, methods, and results. The discussion section will further consider our results in the context of the important role of medical-surgical nurses and error recovery to enhance patient safety.
Background
Patients interacting with healthcare organizations have an expectation of safety. Yet, the fundamental mission of the health profession has been challenged with widespread and persistent medical errors. An estimated 98,000 fatalities result from medical errors every year in the United States (IOM, 2000). In addition to causing loss of public confidence, these events have increased patient morbidity and mortality and raised healthcare costs (Pham et al., 2012). The past 10 years have demonstrated a national focus on reducing these adverse events, with an increase in research and prevention. Despite focused efforts on error prevention, minimal progress has been made to make healthcare safer (MacDonald, 2013).
Error Recovery
...humans are the critical element of the error recovery process. Building on human factors theories, the Eindhoven Incident Causation Model suggested that errors result from technical, organizational, or human failures (van der Schaaf, 1992). Although the model is one of incident causation, it also proposes that errors can be prevented by adequate system defenses (van der Schaaf & Kanse, 2000). When built-in system defenses are unable to control failures, the flexibility, experience, and intuition of the human operator must stop the unintended chain of events before harm occurs. In this sense, humans are the critical element of the error recovery process (Reason, 2008).
The phenomenon of error recovery as a critical defense against medical errors is relatively new, and the mechanisms involved in the recovery process are not well known (Gaffney et al., 2016). The recovery process is defined as the feature of the human system component to detect, localize, and correct system failures (van der Schaaf & Kanse, 2000). The recovery process consists of three sequential phases. First, an error must be detected. The identification or detection of the error is the process of knowing that an error occurred. Error detection can be facilitated by use of an attentional tool such as a checklist, a process (e.g., a double-checking protocol), or by failing to achieve an expected outcome (Jeffs, Lingard, Berta, & Baker, 2012). Familiarity with all aspects of the care plan allows nurses to anticipate and identify potential medical errors.
The recovery process... emphasizes the importance of professional decision-making and clinical reasoning as an expected behavior of nurses.The second phase is intercepting and understanding the nature of the error. In this phase, the nurse attempts to gather an explanation of how the error occurred to prevent it in the future. Finally, the third phase is correcting or counteracting the error. In this phase, the focus is on initiating corrective action to suppress the error by revising the plan or initiating a new plan. Nurses rely on creativity and flexibility to select the most appropriate strategy to interrupt and correct medical errors. The recovery process is the unique difference between patient harm and a near miss and emphasizes the importance of professional decision-making and clinical reasoning as an expected behavior of nurses.
Medical Error Recovery Among Nurses
It is widely accepted that nurses have the most direct contact with patients (Leape, Bates, Cullen, & et al, 1995). When built-in system defenses do not automatically avert potentially dangerous situations, nurses are uniquely poised and possess competencies to identify, interrupt, and correct medical errors. Such instances are referred to as a near miss, preventable error, or recovered medical error.
To date, a small body of research has provided evidence that nurses working in specialty areas successfully recover medical errors and prevent or mitigate patient harm. Dykes, Rothschild, and Hurley (2010a) estimated that critical care nurses recovered, on average, one error per week. Operating room nurses recovered an average of 11 errors per procedure (Yang et al., 2012).
Further insight is needed into the nurse role in error recovery and factors that influence the recovery process. A substantial body of knowledge has indicated that nurses’ ability to provide safe and efficient care is influenced by individual characteristics, including expertise, experience, education, and personality traits (Aiken et al., 2011; Kendall-Gallagher, Aiken, Sloane, & Cimiotti, 2011; McHugh et al., 2013; Scott, Sochalski, & Aiken, 1999). Nursing expertise, comprised of years of nursing experience as well as experiential and practical knowledge, influences nurses’ clinical reasoning skills and quality of care (Benner, 1984; McHugh & Lake, 2010). Nurses gain experience as they are socialized into the profession. They may pursue additional formal education, seek additional training in a practice area, obtain certification, and become recognized experts in a specialty. Along this journey, nurses develop greater confidence and a capacity to recognize patterns and synthesize information. A variety of characteristics and conditions may strengthen or weaken a nurse’s ability to detect and correct errors, yet no studies have explored the relationship between individual characteristics and recovered medical errors.
Personality has been cited as an important influence on general nursing performance (Ellershaw, Fullarton, Rodwell, & McWilliams, 2015; Scheepers, Lombarts, van Aken, Heineman, & Arah, 2014). Conscientiousness and openness are personality traits that have been linked to high performers. The trait of openness is comprised of creativity and adaptability. In turn, creativity and flexibility are strategies that nurses use to correct medical errors, yet no studies have explored the relationship between personality traits and recovered medical errors (Henneman, Blank, Gawlinski, & Henneman, 2006).
Organizational factors, such as the presence of a safety culture and workload, have been demonstrated to influence patient safety (Aiken et al., 2011; Kane, Shamliyan, Mueller, Duval, & Wilt, 2007). The term safety culture is commonly used to describe employers or workers taking a committed, proactive approach toward safety problems to reduce patient harm (Clark, Belcheir, Strohfus, & Springer, 2012). In organizations with strong safety cultures, medical errors are recovered more readily (Kanse, van der Schaaf, Vrijland, & van Mierlo, 2006). The Magnet® Recognition Program offers a framework with established effectiveness for the delivery of safe, high-quality nursing care (Aiken, Buchan, Ball, & Rafferty, 2008; McHugh et al., 2013; Valentine, Murphy, DeRoberts, & Lyman, 2012). For this study, we defined a safety culture as Magnet® designation.
Medical-surgical nurses are challenged with complex workloads, managing five to six interventions for as many as 10 different conditions during a shift (Hanink, 2010). Workload, defined as nurse-to-patient ratio in this study, has been found to be one of the most consistent factors influencing patient outcomes (Aiken et al., 2011; de Cordova, Phibbs, Schmitt, & Stone, 2014; Dunton, Gajewski, Klaus, & Pierson, 2007). While examining medication error interception practices, however, Flynn and colleagues found no association between recovered medical errors and workload among medical-surgical nurses (Flynn, Liang, Dickson, Xie, & Suh, 2012).
Research related to medical errors has grown in the past 15 years and has focused on causation rather than the phenomenon of recovery. Available information regarding the relationship between influencing factors and recovered medical errors is inherent in research focused more broadly on patient outcomes. While existing literature has indicated that nurses recover the majority of medical errors, as compared to other healthcare professionals, there is little information focusing on the nurse role in error recovery. No studies have examined the relationship among individual characteristics, organizational factors, and recovered medical errors (Rothschild et al., 2005). Further insight is needed into the nurse role in error recovery and factors that influence the recovery process.
Aims
Several research questions guided this study. For medical-surgical nurses in hospitals:
- What is the relationship between individual nurse characteristics and recovered medical errors (age, experience, education, expertise, certification, and personality)?
- What is the relationship between organizational factors and recovered medical errors (Magnet® designation and workload)?
- Which individual nurse characteristics or organizational factors predict medical error recovery (age, experience, education, expertise, certification, personality, Magnet® designation, or workload)?
Study Methods
Design, Setting, and Sample
This was a descriptive, correlational study with a cross-sectional design. We used survey data from medical-surgical nurses working in hospitals. Nurses were recruited through two mechanisms; a four-hospital healthcare system in a mid-Atlantic state and a professional nurses association. Inclusion criteria required current employment as a medical-surgical nurse in a hospital. Nurses who were unable to read and write in English were excluded.
The sample size for the study was estimated based on regression analysis with 10 predictor variables (Tabachnick, 2007). We calculated a minimum sample size of 150 as sufficient to provide a medium effect size (R2 = 0.13) with a power of .80 and significance level of .05.
Data Collection
This study was reviewed by the University Office of Research Integrity and Assurance and the healthcare system Research Review Committee and categorized as exempt from Institutional Review Board (IRB) review. Researchers collected data online from October 2014 to January 2015 using Qualtrics® web-based software and a self-report survey tool. Consent was considered completion of the survey. A link to the survey and follow-up reminders were emailed to nurses, using a modified Dillman method (Dillman, 2009).
Measures and Variables
Participants completed three items. These items include demographic questionnaire developed by the investigator, the Recovered Medical Error Inventory (RMEI) (Figure 1) and the Ten-Item Personality Inventory (TIPI) (Dykes, Rothschild, & Hurley, 2010b; Gosling, Renfrow, & Swann, 2003).
Figure 1. Sample Questions from the Recovered Medical Error Inventory
|
Medical record data were not reviewed to learn background information or recommendations about a patient’s treatment plan; e.g. not reading consultant’s suggestions or not knowing of a condition listed in the medical record that would contraindicate giving a typical medication used for presenting symptoms.
Electrolyte replacement was not ordered correctly.
A decision to transfer a patient to an environment lacking clinically required expertise was considered unsafe; e.g. an unstable patient from the CCU to a medical unit; not scheduling a patient for the surgical ICU after complicated surgery; ordering diagnostic testing to be done at a remote site.
|
Outcome Variable. The dependent variable, recovered medical errors, was measured using the RMEI; a 25-item self-report survey (Dykes et al. 2010a). Participants were asked to report the frequency of medical errors recovered over the past three months as (1) none, (2) once, (3) 2-5 times, and (4) over 5 times. The higher the score, the more errors were recovered. The RMEI previously demonstrated an acceptable reliability (0.90) with subscale reliability ranging from 0.75 (Poor Judgment subscale) to 0.88 (Mistake subscale).
Independent Variables. Personality was measured using the Ten-Item Personality Inventory (TIPI). The 10-item, self-report survey measures broad personality domains (Gosling et al., 2003). Using a 7-point Likert scale, participants rated the extent they agreed or disagreed with statements concerning their personality. Possible responses ranged from 1) disagree strongly to (7) agree strongly. Reliability for the TIPI domains ranged as follows: (1) Extraversion (0.68), (2) Agreeableness (0.40), Conscientiousness (0.50), Emotional Stability (0.73), and Openness (0.45). The TIPI has been tested with undergraduate students in multiple countries and has an average correlation of 0.72 across the five domains (Jonason, Teicher, & Schmitt, 2011).
Individual characteristics examined were age, hospital tenure, specialty tenure, education, expertise, certification, and personality. Individual characteristics examined were age, hospital tenure, specialty tenure, education, expertise, certification, and personality. Age, hospital tenure, and specialty tenure were measured on a continuous scale of years and collapsed for further analysis. Nurses reported their highest nursing education degree as a diploma, associate degree, baccalaureate, masters, or doctorate (DNP or PhD). These categories were collapsed for further analysis. Nurses self-reported their level of expertise as novice, competent, or expert.
Organizational factors examined were culture of safety and workload. Participants were asked to indicate if they worked at a Magnet® designated organization. Further, participants reported workload by indicating their typical nurse-to-patient ratio over the past three months. These categories were collapsed for further analysis.
Data Analysis
Data analysis was conducted using the SPSS version 23 (SPSS Inc., Chicago, IL, USA) and Stata SE, version 12.1 (StataCorp, College Station, TX, USA). RMEI frequency counts of errors were determined from category definitions as specified by the tool: (1) none = 0, (2) once = 1, (3) 2 to 5 times = 3 and more than 5 times = 6 and then summed. TIPI items 2, 4, 6, 8 and 10 were reverse coded, and averages were calculated to measure the five personality domains.
RMEI results are characterized descriptively by mean (M), median (Mdn) and interquartile range (IQR). Bivariate relationships between the dependent variable (RMEI) and continuous or ordinal independent variables were evaluated using Spearman nonparametric rank correlations. Kruskal-Wallis nonparametric ANOVA was performed to examine relationships between RMEI and categorical independent variables. A multivariable regression model was calculated to evaluate the independent effects of variables on recovered errors. Various count regression models were considered, including Poisson, negative binomial, and zero-inflated models. A negative binomial model provided the best fit. Incidence rate ratios (IRR) were calculated to assess relationships between RMEI and independent variables. IRR represents the ratio of two group-level RMEI incidences (i.e., the number of recovered medical errors over the three-month RMEI-defined period).
Results
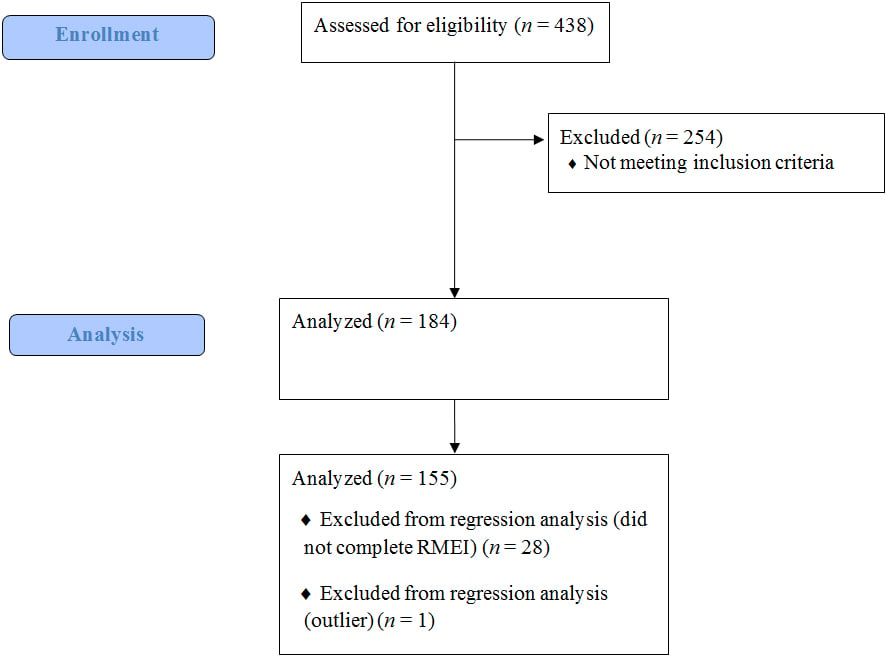
A total of 438 surveys were returned from the 4000 surveys sent indicated a response rate of 10.95%. Of the 438 returned surveys, 254 were excluded because participants answered that they were not employed as a medical-surgical nurse. A total of 184 surveys were eligible for analysis to examine relationships among study variables. Of the 184 eligible surveys, 28 surveys did not contain complete RMEI data and were excluded from regression analysis (n = 28). During the regression analysis, one outlier was eliminated leaving 155 surveys eligible for regression analysis (Figure 2).
Figure 2. Response rate throughout the recruitment and analysis process.
The mean age of study participants was 43.64 (Mdn = 44, SD = 11) which is similar to the overall nurse population in the country (U. S. Department of Health and Human Services Health Resources and Services Administration, 2010). Approximately two-thirds of participants possessed a university degree (63.6%). The majority of participants had ten or fewer years of experience in their current organization (71.2%), and 55.4% of participants had ten or fewer years of experience in their specialty. The sample demographics are presented in Tables 1 and 2.
Table 1. Sample Demographics
|
Variable |
No. |
% |
|
Sex |
||
| Male | 15 | 8.2 |
| Female | 168 | 91.3 |
|
Employment |
||
| Fulltime | 154 | 83.7 |
| Part time | 15 | 8.2 |
| Per diem | 15 | 8.2 |
|
Role |
||
| Staff nurse | 96 | 52.2 |
| Charge nurse | 49 | 26.6 |
| Manager | 35 | 19.0 |
|
Shift |
||
| Day | 120 | 65.2 |
| Night/Evening | 61 | 33.2 |
|
Hours |
||
| 8 hour | 43 | 23.4 |
| 12 hour | 138 | 75.0 |
|
Hospital Size |
||
| Less than 50 beds | 10 | 5.4 |
| 50 beds and greater | 161 | 87.5 |
|
Teaching Hospital |
||
| Yes | 109 | 59.2 |
| No | 62 | 33.7 |
Note. N = 184
Table 2. Sample Individual and Organizational Characteristics
|
Variable |
No. (%) |
M (Mdn) |
SD |
|
Age (in years) |
43.64 (44) |
11.19 |
|
| 20 to 29 | 22 (12.0) | ||
| 30 to 39 | 44 (23.9) | ||
| 40 to 49 | 54 (29.3) | ||
| 50 to 59 | 45 (24.5) | ||
| 60 and above | 15 (8.2) | ||
|
Education |
|||
| Diploma | 3 (1.6) | ||
| Associate | 64 (34.8) | ||
| Baccalaureate | 82 (44.6) | ||
| Master | 33 (17.9) | ||
| Doctor | 2 (1.1) | ||
|
Facility tenure (in years) |
8.20 (6) |
8.03 |
|
| 1 to 10 | 131 (71.2) | ||
| 11 to 20 | 38 (20.7) | ||
| 21 and above | 15 (8.2) | ||
|
Specialty tenure (in years) |
12.61 (10) |
10.80 |
|
| 1 to 10 | 102 (55.4) | ||
| 11 to 20 | 42 (22.8) | ||
| 21 and above | 26 (14.1) | ||
|
Certified |
|||
| Yes | 76 (41.3) | ||
| No | 108 (58.7) | ||
|
Perceived expertise |
|||
| Novice | 9 (4.9) | ||
| Competent | 91 (49.5) | ||
| Expert | 82 (44.6) | ||
|
Magnet® |
|||
| Yes | 65 (35.3) | ||
| No | 115 (62.5) | ||
|
Patient Ratio |
|||
| ≤ 1:4 | 51 (27.7) | ||
| 1:5 | 68 (37.0) | ||
| ≥ 1:6 | 63 (34.2) |
Note. N = 184
On average, each participant indicated that he or she recovered 22 medical errors during the three-month study period (M = 21.74), Mdn = 16.5, IQR = 7 – 29) and 3,392 medical errors were recovered in total. Over 50% of recovered medical errors were caused by the following five reasons: mismanaged aversive symptoms; absent or missed physical exam; mismanaged coexisting health issues; missed orders for prophylactic measures; and improper precaution technique.
Nurses’ total recovered errors were associated with certain individual characteristics. REMI was significantly higher with increasing education (rs = 0.309, p ≤ 0.001), and expertise (rs = 0.235, p = 0.003) (see Table 3). Baccalaureate level nurses were estimated to have a 1.5 times higher medical error recovery rate (IRR = 1.5, 95% CI: 1.1-1.2, p = 0.016), and masters and doctoral level nurses were estimated to have a 1.9 times higher medical error recovery rate than associate or diploma trained nurses (IRR = 1.9, 95% CI: 1.2-2.9, p ≤ 0.005). Expert nurses were estimated to have over 4 times the medical error recovery rate of novice nurses (IRR = 4.1, 95% CI: 1.9-9.1, p ≤ 0.001). No significant relationships were found between REMI and age, hospital tenure, specialty tenure, certification, or personality. The relationship between education and perceived expertise was not examined.
Table 3. Association of Nurse Characteristics with the Dependent Variable
|
Variable |
Kruskal-Wallis |
Spearman Rank |
| Age | 0.110 | 0.404 |
| Education | ≤0.001* | ≤0.001* |
| Hospital tenure | 0.847 | 0.870 |
| Specialty tenure | 0.831 | 0.731 |
| Certified | 0.064 | 0.064 |
| Perceived expertise | 0.003* | 0.003* |
| Personality | ||
| Extraversion | 0.067 | 0.181 |
| Agreeableness | 0.351 | 0.710 |
| Conscientiousness | 0.084 | 0.840 |
| Emotional stability | 0.105 | 0.464 |
| Open to new experiences | 0.853 | 0.789 |
Note. N = 184, *p ≤ 0.01
One organizational factor was related to the dependent variable. There was a moderate inverse relationship between recovered medical errors and the patient ratio (rs = -0.280, p ≤ 0.001), indicating that nurses with higher patient ratios recovered fewer errors. Patient ratio was not significantly associated with RMEI in multivariable regression. Magnet® designation was not associated with recovered medical errors.
Discussion
Results of this study demonstrate the important role of medical-surgical nurses in patient safety. Medical-surgical nurses recovered a total of 3,392 errors over the course of three months, which could potentially equal as many as 13,568 medical errors prevented each year.
This study illustrates nurses’ important role in error recovery and offers further support for seamless academic progression models in order to positively impact patient safety. A growing body of evidence indicates that a higher level of nursing education is associated with better patient outcomes (Aiken et al., 2011; Aiken, Clarke, Cheung, Sloane, & Silber, 2003; Dunton et al., 2007). Our results indicated a significant relationship between education and recovered medical errors. Specifically, university prepared nurses were more likely to recover medical errors and mitigate patient harm than associate and diploma prepared nurses. Nurses provide ongoing assessment and surveillance to detect subtle changes in patient status and prevent complications. Critical thinking is widely considered a hallmark of university education and an important factor in safeguarding patients in today’s complex healthcare environment. This study illustrates nurses’ important role in error recovery and offers further support for seamless academic progression models in order to positively impact patient safety.
...care models leveraging nursing expertise and facilitating transfer of knowledge should be explored to improve patient safety. Expert nursing practice requires complex decision-making in uncertain environments (Bobay, Gentile, & Hagle, 2009). A significant relationship was found between self-reported nursing expertise and recovered medical errors. Nurses’ self-reported level of expertise strongly correlated with peer assessments (as cited in McHugh & Lake, 2010). Medical-surgical nurses who rated themselves as expert practitioners in this study were four times more likely to recover medical errors than self-reported novice nurses. Expert nurses exhibit exceptional clinical reasoning skills consisting of holistic nursing knowledge, skilled know-how, and knowledge of the patient (Henneman et al., 2006). Further, expert nurses are more likely to recognize patterns and rapidly synthesize information. Given the accelerated knowledge base required of nurses today, care models leveraging nursing expertise and facilitating transfer of knowledge should be explored to improve patient safety.
It is widely accepted that workload is an important influence on patient outcomes (Aiken et al., 2011; Kutney-Lee, Lake, & Aiken, 2009). A study of error handling processes in two Dutch hospitals found that heavy workload negatively impacted nurses’ ability to recover medical errors (Habraken & van der Schaaf, 2010). This study indicated a modest inverse relationship between recovered medical errors and workload. Given the acuity, complexity, and rapid turnover of patients on medical-surgical units today, nurses with higher patient loads may experience greater cognitive workloads and be less able to provide the vigilance needed to recover errors.
When a culture of safety is a high organizational priority, staff are continually vigilant in recognizing and resolving safety issues (Rothschild et al., 2005). Magnet® designation has been associated with professional practice environments producing better patient outcomes (Aiken et al., 2008; Kelly, McHugh, & Aiken, 2012; McHugh et al., 2013). Further, professional practice environments have been associated with safer patient care (Flynn et al., 2012). In this study, Magnet® designation and recovered medical errors were not associated. This finding may be due to Magnet® designation as a broad measure and not a specific unit-based measure.
... patients’ interests are best served when nurses use skills that incorporate a higher level of knowledge and judgment. Practice environments must ensure that nurses are socialized to use clinical reasoning and decision-making to create optimal outcomes for patients, both factors discussed in the context of full scope of RN practice. As such, organizations must remove self-imposed barriers to practice and enable nurses to draw upon their education and postlicensure training to make healthcare environments safer. Findings presented in this study suggested that patients’ interests are best served when nurses use skills that incorporate a higher level of knowledge and judgment. By increasing scientific knowledge and adaptive capacity, nurses are better able to identify, interrupt, and correct medical errors and safeguard patients.
Study Limitations
Low participant response rate was a key limitation to this study. Given the sensitive nature of medical errors and the use of self-report tools, results may be over or under-reported. In addition, respondents who completed the survey may be more engaged in error recovery and again, more likely to bias the findings. Convenience sampling potentially decreases generalizability of these study findings; however, comparisons between study participants and the general nursing workforce revealed similar demographic characteristics and the results are consistent with previous research (Budden, Zhong, Moulton, & Cimiotti, 2013; Dykes et al., 2010a; Wilkinson, Cauble, & Patel, 2011). Finally, the nonexperimental, correlational study design focused on relationships of association only and did not allow for inferences regarding causality of variables.
Conclusion: Implications for Research and Practice
Creating a safer healthcare system will depend on the ability of all nurses to fully use their education, expertise and role to identify, interrupt, and correct medical errors to prevent patient harm.
Creating a safer healthcare system will depend on the ability of all nurses to fully use their education, expertise and role to identify, interrupt, and correct medical errors to prevent patient harm. Further analysis of the impact of individual nurse characteristics and organizational factors on the recovery of medical errors is needed. Findings from this study suggested additional areas for future research, such as how workload impacts medical error recovery, what is the relationship between nursing role and medical error recovery, what organizational factors increase error recovery by nurses and what is the relationship between informal education and error recovery.
Our study indicated that expert nurses, and those with advanced education, were better able to identify, interrupt, and recover errors. While advanced education can be achieved via graduate-level degrees, these degrees are not required for all nurses to advance their education, and thus their potential scope of practice. Experience and expertise gained via lifelong learning of new skills and/or certifications can contribute as well. Finally, this study suggested that nursing workload is important to patient safety, a factor that can be influenced by nurse advocacy and participation in policy at the organizational and legislative advocacy levels.
Greater understanding of individual nurse characteristics and organizational factors that influence error recovery can have important implications for nursing practice. Additional knowledge in these areas can inform administrative and educational practices to foster development of strategies to detect and correct medical errors. Armed with this knowledge and appropriate strategies, organizations can work to decrease medical errors and reduce negative outcomes.
Acknowledgements: The authors received no financial or material support for preparation of this article. Sincere gratitude to Dr. Naomi Lynn Gerber for her assistance with this study and constructive comments in preparing this manuscript.
Authors
Theresa (Terri) A. Gaffney, PhD, MPA, RN
Email: Terri.Gaffney@ana.org
Terri Gaffney, PhD, MPA, RN is a nationally recognized healthcare executive with deep experience helping individuals and organizations realize sustainable growth. Terri is passionate about patient safety and has extensively explored the relationship between nurses, nursing, and safety. She has shared her knowledge on this topic through local, state and national presentations and publications. Terri joined the American Nurses Association in 2011, and as the ANA Vice President for Product Development, she is responsible for translating knowledge into innovative products. She leads a team of fifteen who create innovative products as well as develop content for the ANA online library, conferences, workshops, and digital and broadcast media including the National Nurses Week Webinar. Terri earned a PhD degree at George Mason University; an MPA at Virginia Polytechnic Institute & State University; and a BSN at Virginia Commonwealth University School of Nursing.
Barbara J. Hatcher, PhD, MPH, RN, FAAN
Email: Bhatche3@gmu.edu
Barbara J. Hatcher, PhD, MPH, RN, FAAN, is an experienced healthcare executive, health policy expert, health regulator, researcher, and entrepreneur with more than 40 years of experience. Over the past five years, Dr. Hatcher has been an associate professor of nursing at George Mason University where she teaches courses primarily in health administration and health policy for graduate students. Her health policy teaching efforts have resulted in several innovations, including increased student participation in Washington, DC-area health policy networks and the creation of student-generated health infographics. She currently serves as the coordinator for nursing administration programs in the School of Nursing. Barbara earned a PhD in Nursing at George Mason University; an MPH at University of North Carolina, Chapel Hill; and a BSN at the University of Connecticut.
Renee Milligan, PhD, RN, WHNP-BC, FAAN
Email: rmillig3@gmu.edu
Renee Milligan, PhD, RNC is a clinical professor, a women's health advanced practice nurse (WHNP-BC), and a Fellow in the American Academy of Nursing (FAAN). Dr. Milligan has extensive experience in faculty practice and in grants and project management. She has a long history of working with underserved low-income patients, both as a researcher and a practitioner. Dr. Milligan teaches in the nurse practitioner (NP) and the Doctor of Nursing Practice (DNP) programs. She practices at The Pregnancy Aid Center, a clinic for low-income women, in College Park, Maryland, is coordinator of the DNP and NP programs, and is director of the George Mason Partners in Access to Healthcare (PATH) program and clinician in the satellite MAP clinics. Renee earned a Post-Master's Certificate in Women's Health Care at the University of Rochester; a PhD in Nursing at the University of Maryland; an MA in Nursing Education and a BSN at Ball State University.
Amber W. Trickey, PhD, MS, CPH
Email: amber.trickey@gmail.com
Amber Trickey is a Surgery Epidemiologist and Biostatistician at Inova Fairfax Hospital. She creates, implements, and manages a program of biostatistical and epidemiological services that promote clinical and health services research for the Department of Surgery. Her areas of research expertise include, clinical epidemiology, biostatistics, health services research, and hospital quality and safety. Amber earned a PhD in Epidemiology and an MS in Epidemiology at the University of Texas School of Public Health; and a BS in Biomedical Engineering at Tulane University School of Science and Engineering. She is certified in Public Health and SAS Base Programming.
References
Aiken, L.H., Buchan, J., Ball, J., & Rafferty, A.M. (2008). Transformative impact of Magnet designation: England case study. Journal of Clinical Nursing, 17(24), 3330–3337. doi:10.1111/j.1365-2702.2008.02640.x
Aiken, L.H., Cimiotti, J.P., Sloane, D.M., Smith, H.L, Flynn, L., & Neff, D.F. (2011). Effects of nurse staffing and nurse education on patient deaths in hospitals with different nurse work environments. Medical Care, 49(12), 1047–1053. doi:10.1097/MLR.0b013e3182330b6e
Aiken, L.H., Clarke, S.P., Cheung, R.B., Sloane, D.M., & Silber, J.H. (2003). Educational levels of hospital nurses and surgical patient mortality. JAMA: Journal of the American Medical Association, 290(12), 1617–1623.
American Nurses Association. (2015). Nursing Scope and Standards of Practice (3rd ed). Washington, DC: Author
Aranaz-Andrés, J. M., Aibar-Remón, C., Limón-Ramírez, R., Amarilla, A., Restrepo, F. R., Urroz, O., … Larizgoitia, I. (2011). Prevalence of adverse events in the hospitals of five Latin American countries: Results of the “Iberoamerican Study of Adverse Events” (IBEAS). BMJ Quality & Safety, 20(12), 1043–1051. doi:10.1136/bmjqs.2011.051284
Benner, P. (1984). From novice to expert: Excellence and power in clinical nursing practice. Menlo Park, Calif: Addison-Wesley Pub. Co., Nursing Division.
Bobay, K., Gentile, D., & Hagle, M. (2009). The relationship of nurses’ professional characteristics to levels of clinical nursing expertise. Applied Nursing Research, 22(1), 48–53. doi:10.1016/j.apnr.2007.03.005
Budden, J., S., Zhong, E., H., Moulton, P., & Cimiotti, J., P. (2013). Highlights of the National Workforce Survey of Registered Nurses. Journal of Nursing Regulation, 4(2), 5–14.
Clark, C. M., Belcheir, M., Strohfus, P., & Springer, P. J. (2012). Development and description of the culture/climate assessment scale. Journal of Nursing Education, 51(2), 75–80 6p. doi:10.3928/01484834-20111230-01
de Cordova, P. B., Phibbs, C., S., Schmitt, S., K., & Stone, P., W. (2014). Night and day in the VA: Associations between night shift staffing, nurse workforce characteristics, and length of stay. Research in Nursing & Health, 37(2), 90–97. http://doi.org/10.1002/nur.21582
Dillman, D. A. (2009). Internet, mail, and mixed-mode surveys: The tailored design method (3rd ed). Hoboken, N.J: Wiley & Sons.
Dunton, N., Gajewski, B., Klaus, S., & Pierson, B. (2007). The relationship of nursing workforce characteristics to patient outcomes. Online Journal of Issues in Nursing, 12(3).
Dykes, P. C., Rothschild, J. M., & Hurley, A. C. (2010a). Medical errors recovered by critical care nurses. The Journal of Nursing Administration, 40(5), 241–246. doi:10.1097/NNA.0b013e3181da408e
Dykes, P. C., Rothschild, J. M., & Hurley, A. C. (2010b). Recovered medical error inventory. Journal of Nursing Scholarship, 42(3), 314–318. doi:10.1111/j.1547-5069.2010.01356.x
Ellershaw, J., Fullarton, C., Rodwell, J., & Mcwilliams, J. (2015). Conscientiousness, openness to experience and extraversion as predictors of nursing work performance: a facet-level analysis. Journal of Nursing Management, 23(4), 1–93. doi:10.1111/jonm.12306
Flynn, L., Liang, Y., Dickson, G., L., Xie, M., & Suh, D.C. (2012). Nurses’ Practice Environments, Error Interception Practices, and Inpatient Medication Errors. Journal of Nursing Scholarship, 44(2), 180–186. doi:10.1111/j.1547-5069.2012.01443.x
Gaffney, T. A., Hatcher, B. J., & Milligan, R. (2016). Nurses’ role in medical error recovery: An integrative review. Journal of Clinical Nursing, 25(7/8), 906–917 12p. doi:10.1111/jocn.13126
Gosling, S., Renfrow, P., & Swann, W. (2003). A very brief measure of the big five personality domains. Journal of Research in Personality, 37(6), 504–528.
Habraken, M. M. P., & van der Schaaf, T. W. (2010). If only....: Failed, missed and absent error recovery opportunities in medication errors. Quality & Safety In Health Care, 19(1), 37–41. doi:10.1136/qshc.2007.026187
Hanink, E. (2010). Medical-surgical nursing. Variety: The spice of this specialty. Working Nurse. Retrieved from http://www.workingnurse.com/articles/Medical-Surgical-Nursing
Helmreich, R. L. (2000). On error management: Lessons from aviation. BMJ (Clinical Research Ed.), 320(7237), 781–785.
Henneman, E., Blank, F., Gawlinski, A., & Henneman, P. (2006). Strategies used by nurses to recover medical errors in an academic emergency department setting. Applied Nursing Research, 19(2), 70–77.
Institute of Medicine. (2000). To err is human: building a safer health system. Washington, D.C: National Academy Press.
Jeffs, L. P., Lingard, L., Berta, W., & Baker, G. R. (2012). Catching and correcting near misses: The collective vigilance and individual accountability trade-off. Journal Of Interprofessional Care, 26(2), 121–126. http://doi.org/10.3109/13561820.2011.642424
Jonason, P., Teicher, E., & Schmitt, D. (2011). The TIPI’s validity confirmed: Associations with sociosexuality and self-esteem. Individual Differences Research, 9(1), 52–60.
Kane, R., Shamliyan, T., Mueller, C., Duval, S., & Wilt, T. (2007). The association of registered nurse staffing levels and patient outcomes. Systematic review and meta-analysis. Medical Care, 45(12), 1195–1204.
Kanse, L., van der Schaaf, T. W., Vrijland, N. D., & van Mierlo, H. (2006). Error recovery in a hospital pharmacy. Ergonomics, 49(5–6), 503–516.
Kelly, L. A., McHugh, M. D., & Aiken, L. H. (2012). Nurse outcomes in Magnet® and non-Magnet hospitals. The Journal Of Nursing Administration, 42(10 Suppl), S44–S49. doi:10.1097/NNA.0b013e31822eddbc.
Kendall-Gallagher, D., Aiken, L., Sloane, D., & Cimiotti, J. (2011). Nurse specialty certification, inpatient mortality, and failure to rescue. Journal of Nursing Scholarship, 43(2), 188–194. doi:10.1111/j.1547-5069.2011.01391.x
Kutney-Lee, A., Lake, E., & Aiken, L. (2009). Development of the hospital nurse surveillance capacity profile. Research in Nursing & Health, 32(2), 217–228. doi:10.1002/nur.20316
Landrigan, C. P., Parry, G. J., Bones, C. B., Hackbarth, A. D., Goldmann, D. A., & Sharek, P. J. (2010). Temporal trends in rates of patient harm resulting from medical care. The New England Journal of Medicine, 363(22), 2124–2134. doi:10.1056/NEJMsa1004404
Leape, L.L., Bates, D.W., Cullen, D.J., & et al. (1995). Systems analysis of adverse drug events. JAMA, 274(1), 35–43. http://doi.org/10.1001/jama.1995.03530010049034
MacDonald, I. (2013, September 20). Hospital medical errors now the third leading cause of death in the U.S. Retrieved from http://www.fiercehealthcare.com/story/hospital-medical-errors-third-leading-cause-death-dispute-to-err-is-human-report/2013-09-20
McHugh, M.D., Kelly, L.A., Smith, H.L., Wu, E.S., Vanak, J. M., & Aiken, L.H.. (2013). Lower mortality in magnet hospitals. Medical Care, 51(5), 382–388. doi:10.1097/MLR.0b013e3182726cc5
McHugh, & Lake. (2010). Understanding clinical expertise: Nurse education, experience, and the hospital context. Research in Nursing & Health, 33(4), 276–287. doi:10.1002/nur.20388
Pham, J. C., Aswani, M. S., Rosen, M., Lee, H., Huddle, M., Weeks, K., & Pronovost, P. J. (2012). Reducing medical errors and adverse events. Annual Review of Medicine, 63, 447–463. doi:10.1146/annurev-med-061410-121352
Reason, J. (1990). Human error. Cambridge, UK; New York: Cambridge University Press.
Reason, J. T. (2008). The human contribution: Unsafe acts, accidents and heroic recoveries. Farnham, England; Burlington, VT: Ashgate.
Rothschild, J.M., Langrigan, C.P., Cronin, J.W., Kaushal, R., Lockley, S.W., Burdick, E., … Bates, D.W. (2005). The critical care safety study: The incidence and nature of adverse events and serious medical errors in intensive care. Critical Care Medicine, 33(8), 1694–1700.
Scheepers, R. A., Lombarts, K. M. J. M. H., van Aken, M. A. G., Heineman, M. J., & Arah, O. A. (2014). Personality Traits Affect Teaching Performance of Attending Physicians: Results of a Multi-Center Observational Study. PLoS ONE, 9(5), e98107. doi:10.1371/journal.pone.0098107
Scott, J. G., Sochalski, J., & Aiken, L. (1999). Review of magnet hospital research: findings and implications for professional nursing practice. The Journal Of Nursing Administration, 29(1), 9–19.
Tabachnick, B. G. (2007). Using multivariate statistics (5th ed). Boston: Pearson/Allyn & Bacon.
U. S. Department of Health and Human Services Health Resources and Services Administration. (2010, September). The Registered Nurse Population: Findings from the 2008 National Sample Survey of Registered Nurses. US Department of Health and Human Services. Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnsurveys/rnsurveyfinal.pdf
Valentine, N. M., Murphy, D., DeRoberts, A., & Lyman, M. B. (2012). The nursing quality partnership: Building a health system approach to improving care in community hospitals using principles of the magnet program of excellence. Nursing Administration Quarterly, 36(4), 340–352. doi:10.1097/NAQ.0b013e318266946a
van der Schaaf. (1992). Near miss reporting in the chemical process industry. Eindhoven University, Netherlands.
van der Schaaf, T. W., & Kanse, L. (2000). Errors and error recovery. In P. F. Elzer, R. H. Kluwe, & B. Boussoffara (Eds.), Human Error and System Design and Management (Vol. 253, pp. 27–38). Godalming: Springer-Verlag London Ltd.
Wilkinson, W., Cauble, L., & Patel, V. (2011). Error detection and recovery in dialysis nursing. Journal Of Patient Safety, 7(4), 213–223. doi:10.1097/PTS.0b013e3182388d20
Yang, Y. T., Henry, L., Dellinger, M., Yonish, K., Emerson, B., & Seifert, P. C. (2012). The circulating nurse’s role in error recovery in the cardiovascular OR. AORN Journal, 95(6), 755–762. doi:10.1016/j.aorn.2011.09.022