


Reaching disenfranchised clients who are either underinsured or who have no insurance presents unique challenges for healthcare providers and organizations. To reach clients experiencing disparities in healthcare access, a social determinant of health, innovative models of healthcare delivery must be developed. The Juntos for Better Health project directly focused on the social determinant of lack of access to care for prevention and treatment of diabetes, depression, and obesity. In the article, we discuss the background that provided the framework for this project, reviewing literature related to mobile vans and traveling nurses, and then describe the geographical traveling healthcare team setting. The article discusses the Juntos for Better Health project, including several phases of implementation, services of the traveling healthcare team delivery system, and partnerships that included four healthcare providers and a state university in a United States-Mexico border town located in Texas. Partnering agencies included a community-based federally qualified healthcare center, the local state mental health authority, the city health department, and the local drug treatment agency. The conclusion briefly describes plans for the future.
Key Words: Mobile Traveling Healthcare Teams, Integrated Behavioral Healthcare, consortiums, collaborative, partnerships
Reaching disenfranchised clients who are either underinsured or have no insurance presents unique challenges for healthcare providers and organizations. Reaching disenfranchised clients who are either underinsured or have no insurance presents unique challenges for healthcare providers and organizations. Adler et al., (2016) addressed the importance of understanding social determinants of health (SDOH) whereby access to education, transportation, and addressing basic economic needs lead to long term health outcomes. Higher levels of educational attainment are positively related to life expectancy and higher rates of child health, as well as lower rates of chronic disease (e.g., diabetes) and infant mortality (Braveman & Gottlieb, 2014). Egerter, Braveman, Sadegh-Nobari, Grossman-Kahn, & Dekker (2011) proposed that education affects health through health knowledge and literacy, which lead to better quality diets, more exercise, and lower likelihoods of conditions such as diabetes, depression, and obesity. Additionally, for the elderly population, access to vaccinations are greatly related to social factors such as income (i.e., perceptions of affordability); access to transportation; and sources of medical information available to patients.
... delivery systems need to address access by going where clients live and work. According to Mandel (2014), some reasons for disparities in access to healthcare are: lack of health insurance; health insurance plans that limit the amount of services; irregular sources of care; use of clinics and emergency rooms without case management; legal obstacles (e.g., Medicaid unavailable for immigrants with residency of less than five years); structural barriers (e.g., inconvenient appointment times, lengthy wait times; lack of healthcare providers; and language and cultural barriers (e.g., poor communication skills by client and provider). To reach clients experiencing disparities in healthcare access, innovative models of healthcare delivery must be developed. To address the challenges identified by Mandel (2014), delivery systems need to address access by going where clients live and work. The delivery system must also address both primary and behavioral health needs of clients, with an emphasis on prevention and chronic disease management. Collaboration among multiple agencies is truly needed to provide comprehensive care in a cost effective manner.
This article provides a roadmap for a unique collaboration among four healthcare providers and a state university in a United States (US)-Mexico border town located in Texas. The collaborating agencies include a community-based federally qualified healthcare center (FQHC); the local state mental health authority (LMHA); the city health department; and the local drug treatment agency. The consortium is funded by Methodist Healthcare Ministries (MHM) with a grant from the Social Innovative Fund (SIF) and the Meadows Foundation. The long-term goal of this project, called Juntos (meaning “together”) for Better Health, is to develop a consortium where resources and best practices are shared. The consortium provides a continuum of care with navigators providing case management and linkage to a medical home with a common data sharing information system.
The Juntos for Better Health project focuses on access to care for prevention and treatment of diabetes, depression, and obesity. The Juntos for Better Health project focuses on access to care for prevention and treatment of diabetes, depression, and obesity. The project has various components including: patient education; addition of personnel to increase access for underserved clients; a study to determine the effectiveness of a structured call center protocol for engaging clients who have missed appointments; and mobile traveling healthcare teams (THCTs) to conduct initial primary and behavioral assessments with linkage to a medical home. The THCTs are mobile integrated behavioral health (IBH) teams which carry all supplies and equipment in folding wagons and establish clinics in available spaces. Examples of clinic sites have been libraries, breakrooms, kitchens, and other spaces which meet the project criteria for safety and privacy.
This model differs significantly from mobile vans. The Juntos THCTs rely on the trust that the agency personnel has established with clients to overcome initial barriers of mistrust a client may have with the team. To understand the unique nature of the Juntos THCT delivery model, a brief review of the literature related to mobile vans and traveling nurses as established by the North Carolina Public endeavor will be presented. The THCT delivery system was developed to overcome some of the barriers to mobile van utilization as described in the literature. This article will also describe the setting for the Juntos project and provide a detailed description of the Juntos THCT delivery system.
Background
Frontier Nursing: History of Public Health Nursing in North Carolina
Nursing has a rich history of providing care in the homes and communities of clients. Nursing has a rich history of providing care in the homes and communities of clients. Lillian Wald, who established the Henry Street Nursing Settlement in 1893, provided nursing care to clients in their homes and the neighborhoods of the poor and immigrant communities of New York. Public health nursing in North Carolina had its roots in civic and church organizations who hired nurses to visit the sick. Amelia Lawson was the first public health nurse to practice in North Carolina in 1904 (Ehrenfeld, 1919).
Lydia Holman did not follow the traditional pattern of employment by benevolent associations or local governments. Ms. Holman saw with her eyes and soul the suffering of the poor Appalachian families. For 58 years she traveled on horseback into the backwoods and the mountains of North Carolina. She delivered hundreds of babies; performed minor surgery and dentistry; immunized individuals against typhoid; and fought epidemics of tuberculosis, pellagra, smallpox, and measles (Ehrenfeld, 1919). Mobile vans became the modern day equivalent of the public health nurses on horseback when they embraced the concept of traveling to the communities of underserved clients.
Mobile Vans
Mobile vans became the modern day equivalent of the public health nurses on horseback when they embraced the concept of traveling to the communities of underserved clients. Yu, Hill, Ricks, Bennet, & Oriol (2017) conducted a meta-analysis of 51 articles between January 2015 and December 2016 about the use of mobile healthcare vans. The meta-analysis used PubMed and the online collaborative research network of mobile clinics, MobileHealthMap.org, to access data to assess the strengths and weaknesses of mobile vans. One driving factor in the success of mobile vans was their outreach to vulnerable populations by bringing services to the community. According to Mobile Health Maps data, Mobile Health Clinics (MHC) still provide up to 6.5 million visits a year with a focus on primary care (42%), preventive screenings (45%), and dental services (30%) (Yu et al., 2017). According to Yu et al. (2017), there are approximately 2,000 mobile vans nationwide. The meta-analysis found that MHCs serve as a platform to help clients navigate the complex healthcare system.
The meta-analysis identified common themes. According to Yu et al. (2017), the most common themes were respectively: increasing healthcare access; improving health outcomes; addressing SDOH; advancing population health; reducing healthcare costs; and mobile clinics and healthcare reform (e.g., reimbursement issues). The meta-analysis (Yu et al., 2017) identified the most common barriers to accessing healthcare among both the general and vulnerable populations were transportation; uninsured status; financial costs; linguistic and cultural barriers; lack of healthcare providers; perceived absence of patient-centered care; psychological barriers; intimidation by healthcare settings; hours of operation; and anonymity concerns. Mobile Health Map (2016) identified that 52.2% of clients seen by mobile vans nationwide identified as non-white and 40% identified as Hispanic.
Yu et al. (2017) found that major factors in the success of MHCs was the ability to eliminate many of the above barriers. By delivering necessary services right to clients’ doorsteps, often without fees and complex paperwork, many MHCs are able to serve individuals who may not have the time, resources, and motivation to travel to traditional clinics. However, the key factor was the establishment of a trusting relationship between MHC van personnel and the community leaders and clients in neighborhoods where vans were located.
MHCs go into the community and set up shop at places such as churches, malls, and schools. MHCs are able to bridge the gap between the community and traditional clinics. MHCs go into the community and set up shop at places such as churches, malls, and schools. By bringing healthcare to the community, MHC staff better understand nonmedical factors that impact healthcare behavior. Serving as a bridge between the community and the broader healthcare system, coordination of care is more likely to occur (Yu et al., 2017).
The meta-analysis also identified limitations and challenges created by MHCs. Some potential limitations were the risk of increased fragmentation; issues with finances; constraints by space and clinic structure; and challenges in logistical planning. Fragmentation of care resulted from the limited range of services by MHCs and the lack of linkages to more comprehensive medical homes. Financial issues arose from the cost of maintenance of the mobile van. Studies from the meta-analysis found that mobile mammography vans had financial losses in 52% of cases due to downtime for vehicle maintenance, vehicular problems, bad weather, and equipment damage (Yu et al., 2017). Another problem was the dependency on grants for survival of the vans. All too often services stopped when grant funding ended. For disenfranchised clients, this destroys trust for other endeavors focused on increasing access. Surveyors found that 33% of MHCs reported staffing problems, including recruiting culturally competent community healthcare providers who are comfortable working in small spaces in the community (Yu et al., 2017).
The Juntos THCT model uses the same type of creativity and pioneering spirit that guided public health nursing and the implementation of mobile vans. The THCT combines the mobile van concept and incorporates the nurse on horseback approach to minimize or eliminate barriers and obstacles noted in the literature.
The Traveling Healthcare Team Setting
The Juntos for Better Health project services Webb, Zapata, and Jim Hogg counties in South Texas. Webb County, with a population of 271,193, is the fourth largest county in the South Texas area (U.S. Census Bureau, 2014). Webb County has high rates of poverty and low levels of education. Over ninety-four percent (94.6%) of residents are Hispanic/Latino. Many constituents in this area are not fully bilingual and speak Spanish as their main language. Residents in this region suffer from disproportionate health disparities which stem from extreme poverty, lower levels of educational attainment, and inadequate access to basic healthcare needs. The education, economic, and language disparities leave a segment of this population with limited understanding, and thus restricted access to resources available in the area.
Poverty is pervasive along the state’s southern border with Mexico, placing border residents at high risk for poor health status. Poverty is pervasive along the state’s southern border with Mexico, placing border residents at high risk for poor health status. According to the U.S. Census Bureau (2014), 31.8% of Webb, 27.9% of Jim Hogg, and 29.1% of Zapata county residents live below the federal poverty level, compared to the state average of 15.6%. Additionally, Webb county is home to more than 60 colonias, defined as unincorporated settlements of land along Texas-Mexico border that may lack some of the most basic living necessities such as drinking water, sewer systems, electricity, paved roads, and safe and sanitary housing. More than 25,000 colonia residents rely on an episodic system of care dependent on funding and strained social programs with limited capacity (U.S. Census Bureau, 2014).
According to the most recent community needs assessment, the use of preventive healthcare services is low among the general Mexican American population, and Laredo/Webb counties are no exception (Laredo/Webb County Community Needs & Workforce Assessment, 2013). Laredo and surrounding communities continue to see increasing behavioral health (including mental health, substance abuse, and domestic violence) cases with limited personnel and service-based resources to match the need.
A primary barrier to healthcare is a lack of accessibility to transportation coupled with the region’s significant shortage of physician capacity for both primary care and specialty care in areas such as mental healthcare. According to the Robert Wood Johnson Foundation (2009) and University of Wisconsin Population Health Institute’s County Health Rankings & Roadmaps (2015), Texas has one mental health provider for 1,070 residents. Webb county has one provider for every 3,970 residents. This shortage of behavioral health providers demands the most efficient use of services throughout the region. The current delivery model is designed to react to clients with chronic conditions at the hospital and then to treat in the hospital setting.
Diabetes is epidemic in the Juntos for Better Health project service region. The 2015 Texas Department of State Health Services health facts profile showed the diabetes mortality in Webb county at almost twice the rate of the State of Texas (38.0 per 100,000 v. 21.6 per 100,000). According to the Centers for Disease Control and Prevention, adult diabetes prevalence has grown from 6.2% of the adult population in 1999 to 9.4% of the adult population in 2015 (Texas Department of State Health Services, 2015).
The Juntos for Better Health project was designed to develop a consortium that provides connectivity between community-based interventions and medical homes.The lack of public health infrastructure in Webb county further exacerbates challenges in accessing high-quality primary and mental health services. There is a need for greater connectivity and coordination among hospital and primary care providers and community-based chronic disease management resources so that clients are able to learn and have support for lifestyle changes to effectively improve outcomes. The Juntos for Better Health project was designed to develop a consortium that provides connectivity between community-based interventions and medical homes.
The Juntos for Better Health Project
The Beginning Phase
Methodist Healthcare Ministries received a Social Innovation Grant in 2014 to address the epidemic problems of diabetes, depression, and obesity in 14 South Texas counties. Methodist Healthcare Ministries then developed a Request for Application (RFA) for agencies in South Texas to develop and submit proposals. Nine proposals funded by MHM used innovative strategies to address prevention and care for diabetes, depression, and obesity using an integrated behavioral health model (IBH); the nine proposals became the Sí Texas project. The Juntos for Better Health project was funded through this RFA in 2016. The Meadows Foundation began funding the Juntos project in 2017; total funding for the Juntos project ranged from 3.4 million to 4.2 million dollars per year.
All of the funded proposals in the Sí Texas portfolio committed to collect core measures. The core measures were assessment of mental health (PHQ-9); assessment of quality of life (Duke Health Profile); A1c/glucose levels; body mass index (BMI); and blood pressure. The PHQ-9 (Kroenke, Spritzer, & Williams, 2001) is a nine item depression scale. It is one of the most validated tools in mental health and is a powerful tool to assist clinicians with screening for depression and monitoring treatment response. The Duke Health Profile (Parkerson, Broadhead, & Tse, 1990) is a 17-item generic self-report instrument containing six health measures. The measures are physical, mental, social, general, perceived health, and self-esteem. In addition, the Duke tool assesses for anxiety, depression, pain, and disability.
All Sí Texas projects had to initially identify their beginning level of integration and their outcome goals for level of integration. The six levels of integration were minimal collaboration; basic collaboration at a distance; basic collaboration on-site; close collaboration on-site with some system integration; close collaboration approaching an integrated practice; and full collaboration in transformed/merged integrated practice.
The state university in Laredo, Texas was the lead organization for the Juntos for Better Health projects. The principal investigator for the program met with local chief executive officers (CEOs) from major healthcare agencies that provide primary and behavioral healthcare services to underinsured or uninsured individuals in Laredo. The CEOs of these organizations committed to a collaborative proposal to address the health of persons in Laredo with diabetes, depression, and obesity. The agencies were the LMHA, an FQHC, the city health department, and the local substance abuse agency.
The Juntos for Better Health project used a multi-prong approach to achieve the goal of an integrated and coordinated healthcare system... The Juntos for Better Health program used a multi-prong approach to achieve the goal of an integrated and coordinated healthcare system, thus moving the consortium to a higher level of integration. The first prong focused on patient education and testing a research protocol to determine effectiveness of a structured intervention to re-engage clients who have missed appointments with primary health or behavioral health providers. Prong two focused on shared protocols, services, and personnel from the identified network providers through the mechanism of the mobile Traveling Healthcare Teams (THCT) embedded in the community. This prong moved the consortium integration from a level four (close collaboration on-site with some system integration) to a level six (full collaboration in transformed/merged integrated practice). Prong three focused on providing specific personnel needed by agencies to handle increased patient volume as a result of the THCTs. As noted previously, this article only focuses on the development and evolution of the THCTs.
Initial Implementation of THCTs
In the beginning, the THCT consisted of a mid-level provider (family nurse practitioner or physician assistant); medical assistant; case manager; and licensed professional counselor. All personnel in the first THCT came from the city health department. The first THCT was located in a brick and mortar community center, in downtown Laredo. This site was chosen because of close proximity to downtown stores and the plaza where the local transit system is located. As a result, many uninsured and underinsured individuals gather there daily. Within six-months, a second brick and mortar site was established within close proximity to the area’s oldest flea market in central Laredo. Personnel who comprised the first THCT team rotated between the downtown and central sites. The aim of the THCT at this point was to move into the community where clients live, work, and play. It is important to note that, at this stage in the development of the THCT, all of the personnel were from one agency.
... the THCT is the bridge between the community and the medical home. Prior to the implementation of the first THCT, protocols were developed. Some examples of these protocols include a process for collecting informed consent and demographic information; and procedures for collecting core measures; crisis management and referral for medical or mental health crisis; community outreach and scheduling appointments; and linkage and documentation to a medical home. Trainings and workshops emphasized the role of the THCT in increasing access to services for individuals experiencing barriers to obtaining medical and behavioral care by providing these services directly in the community. THCT services are designed as the entry point into healthcare services, as well triage for clients and referral to the appropriate medical home. In essence, the THCT is the bridge between the community and the medical home. As noted earlier, core measures were (and still are) obtained for all clients of the THCT. This includes demographic information; PHQ-9 and Duke Health Profile screening; glucose testing; height, weight and BMI; blood pressure; and a physical exam.
THCT Services
During the first year of operation, it became apparent that we needed a new model for reaching disenfranchised clients. We identified work flow stations for the THCTs, to manage the flow of clients in an orderly fashion. The first station obtained the institutional review board (IRB)-approved informed consent to participate; demographic information; and PHQ-9 and Duke Health Profile screening assessments. Providers at the second station were responsible for documenting vital signs and other physical measures, such as blood pressure, glucose, height, weight, BMI, and a medical history. The mid-level provider (FNP or PA) operated the third station and conducted the physical assessment. Individual services were concluded when the client returned to station one to receive recommendations for referral to a medical home. At this point, the linkage to the medical home was provided by the case manager, who obtained an appointment with the health department primary care clinic. In the beginning, the entire process was conducted using pen and paper hardcopies. These hardcopies were transmitted to the Juntos for Better Health data analyst who then converted them into digital electronic files. The THCT had support from two coordinators who focused on client recruitment and scheduling.
During the first year of operation, it became apparent that we needed a new model for reaching disenfranchised clients. Utilization of the brick and mortar clinics failed to reach the large number of clients in need of services. Unless clients lived near the clinic, barriers still existed to access the much needed services. During that first year, the THCT saw 242 clients. In addition, it became obvious that having personnel from only one agency was not facilitating the goal of total integration among agency personnel and their resources.
Modifications and Evolution of the Second THCT Model
Brick and mortar clinics were unsuccessful. As a result, we developed totally mobile traveling teams. To secure sufficient clinic sites, a Juntos for Better Health community outreach team was hired to ensure sufficient client volume. This model uses the THCT site administrator to arrange client appointments, with a target goal of 15-18 clients per day. The agency administrator has a trusting relationship with their specific client population, therefore, some barriers related to lack of trust and cultural sensitivity of providers are eliminated with this model. In essence, the THCT provides services to agencies/organizations when they are invited into the “home” of the organization. The Juntos for Better Health THCT joins efforts with the organization to meet their client needs. This approach empowers the organization as an equal partner, and by extension the community as well. This empowerment allows the THCT to leverage the trust that leaders and coordinators of the organizations have with their clients.
Brick and mortar clinics were unsuccessful. As a result, we developed totally mobile traveling teams. Totally mobile traveling teams move into communities carrying with them all of their equipment and supplies. THCT staff is now setting up clinics in lobbies, kitchens, hallways, large conference rooms, and anywhere they can find space. This requires them to also carry privacy screens and become very creative to maximize spaces for efficiency and privacy. Examples of sites are community centers, churches, soup kitchens, emergency shelters, housing authorities, rural colonias, and schools. School sites provide services for parents, grandparents, and other adult family members of the students.
An example of one of the first success stories of the mobile THCT is a local nonprofit organization for needy military veterans and surviving spouses. The organization provides monthly groceries, personal hygiene, and household items to clients. The THCT scheduled clinics on days when these items were distributed. The first day that the sign-in list was available, it filled and the agency asked for more days. The THCT was overwhelmed by the reception of the organization and its clients. Before the stations were even ready, there were over 20 individuals waiting for services.
Results of the new traveling model compared to the brick-and-mortar model were very different. Results of the new traveling model compared to the brick-and-mortar model were very different. The newly redesigned THCT saw 389 clients during the first two-months of operation. The next step was to add a second mobile THCT that would serve the rural areas of Webb, Jim Hogg, and Zapata counties, which became operational in July 2016. This method of total mobile delivery has developed a strong bond with the community. Over 95 new partnerships with over 190 new sites have been formed. During year three, the newly redesigned mobile THCTs proved to be a success, offering care to just under 5,300 patients.
The New Composition of THCT
The redesigned flow of the stations facilitated the multi-discipline and multi-agency approach. To increase the level of integration among the consortium network providers, the composition of the THCTs was also redesigned. Going totally mobile allows the team to access the community more easily and was the first step of the redesign. In the first year, all THCT staff came from one organization. The target population predominately included people who had not received any medical or mental health services in years. The Juntos for Better Health team began a close assessment of network provider personnel to identify resources that could be shared. Teams were redesigned to focus on different components of the screening process, specifically intake and mental health assessment; vitals and medical history; health assessment; and exit interview. The redesigned flow of the stations facilitated the multi-discipline and multi-agency approach. THCT teams now were IBH (primary care plus mental health) and multi-agency (Figure 1).
Figure 1: Full Integration: Multi-Disciplinary and Multi-Agency Team Composition
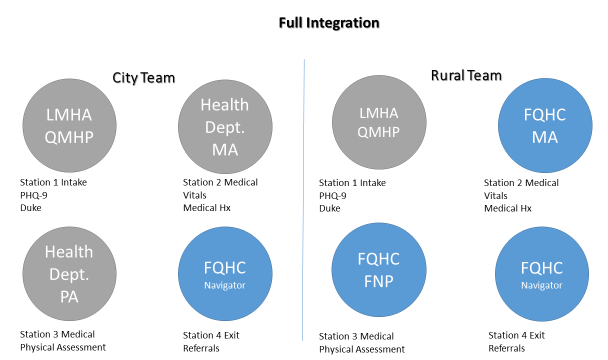
Each THCT was now comprised of staff from the local mental health authority, the city health department, and an FQHC. Stations were now staffed with the following personnel: a qualified mental health professional (QMHP); a medical assistant (MA); an FNP or PA; and an FQHC patient navigator. The (LMHA) handles intake and mental health assessments.
If any mental health issues requiring immediate attention are identified, the process stops and the individual is linked immediately to crisis services. If any mental health issues requiring immediate attention are identified, the process stops and the individual is linked immediately to crisis services. If no immediate mental health needs are identified, services continue. Due to the high number of crises identified at sites, the THCTs now have an onsite crisis worker to reduce delivery time for service. Prior to this, the client had to wait anywhere from one to three hours for the crisis worker to arrive. Over the course of the second year, we made modifications to station flow to maximize efficiency (Figure 2).
Figure 2: Second Station Flow
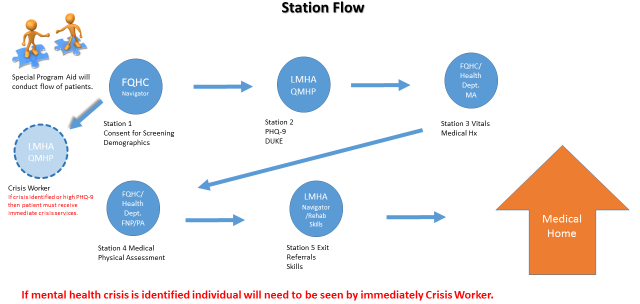
The current THCT composition is a FQHC/ Patient Navigator who handles intake; a LMHA/QMHP who conducts a mental health assessment; a FQHC or health department MA who obtains vital signs and medical history; FQHC or health department FNP or PA who conducts health assessment; and a LMHA/Rehabilitation Skills worker who conducts exit interviews and makes referrals to a medical home, along with an established appointment. The LMHA crisis worker is on site for any crisis situation that may occur and aids with exit interviews when available.
Linkage of Referrals to Medical Homes
During the second year of THCTs, we implemented a shared electronic database... In the first year of the THCT, pen and paper referrals were provided to patients with no shared tracking system in place. During the second year of THCTs, we implemented a shared electronic database that is Health Insurance Portability and Accountability Act (HIPAA) compliant. This shared database allows personnel in station 5 to upload client information and medical home referral to the receiving agency. Since it is a shared drop box, the medical referral is easily accessed and viewed by the receiving agency to include date of appointment.
Referrals to medical homes are tracked by the individual agency patient navigators using the established Juntos for Better Health Referral Follow-up Protocol. This protocol requires an initial referral follow-up call within five business days of receiving the referral. This allows the medical home personnel to introduce themselves to the client and inform him or her that the agency has received the referral. Each contact requires the receiving agency navigator to document the contact and/or inability to reach the client via the shared database.
The IBH coordinator, including the data analyst, monitor and track whether appropriate actions, as per the protocol, have been followed. If appropriate protocols have not been implemented, program leads at each agency are notified. At the end of the month, any major follow-up issues that have occurred are addressed by the compliance officer, who then requests a corrective action plan from the agency.
Conclusion: Next Steps
...Juntos for Better Health project staff are readily available to serve as mentors. In year four, a more structured protocol will be used by the network provider patient navigators who contact THCT clients. This protocol mirrors that used in years two and three for clients who missed appointments. The patient navigators from each organization will conduct phone calls to clients at the university call center. The call center has the capability to capture clients’ reasons (and thus barriers) for failure to follow-up with medical home appointments. By having patient navigators come to the university call center, Juntos for Better Health project staff are readily available to serve as mentors. To increase the capture rate for medical home compliance, the program will use the LMHA, the health department, and the substance abuse agencies to provide transportation for clients to the medical home as needed.
The Juntos for Better Health project focuses specifically on the social determinant of lack of access to care for prevention and treatment of diabetes, depression, and obesity. The roadmap described above addresses methods for overcoming the challenges of mobile vans. While the lessons have been challenging, they have been invaluable in helping to redesign delivery of services to disenfranchised individuals. The new redesigned model can be used by anyone seeking to truly reach clients who encounter access barriers to healthcare.
Acknowledgement: This program was supported in part by: Methodist Healthcare Ministries of South Texas, Inc.; Social Innovation Fund; and The Meadows Foundation.
Authors
Glenda C. Walker, RN, PhD
Email: glenda.walker@tamiu.edu
Glenda C. Walker, Ph.D., Juntos Director and Principal Investigator, assumed the position of Dean of the College of Nursing and Health Sciences in August 2013. She received a PhD in Nursing from the University of Alabama in Birmingham, Alabama. Dr. Walker has received more than $40,312,860 (to include the Juntos) in state and federal funding for research and educational programs and has published over 30 articles in peer reviewed journals as well as chapters in nursing books. In 2013, Dr. Walker published her first book, See Spot Run: Lessons for Life. The book uses metaphors about her family of Dalmatian dogs to illustrate psychiatric and spiritual principles for life. Dr. Walker has extensive experience in the role of a nursing education administrator. She has served as an education administrator in public, private, and health science center nursing programs.
Viviana Martinez-Gómez, MS, LCDC, CART
Email: viviana.martinez@tamiu.edu
Viviana Martinez-Gomez is a clinician, program director, and consultant with experience in the substance abuse field specializing in interventions in Laredo, Texas. Ms. Martinez earned a Master’s Degree in Criminology and Sociology from Texas A&M International University in Laredo, Texas and is a Licensed Chemical Dependency Counselor and Certified Anger Resolution Therapist. Ms. Martinez is currently working on a Doctorate degree in Organizational Leadership from Northcentral University. Her research interests include cultural competency, trust among collaborators, and collaborative partnerships. She is a Program Director at Texas A&M International University overseeing a research study for non-compliant patients with Diabetes and/or Depression and integrated health programs looking at best practices.
Roberto O. Gonzalez, MS
Email: roberto.gonzalez@tamiu.edu
Roberto Gonzalez was born and raised in Laredo. He attended Laredo public schools and graduated from Martin High School. Mr. Gonzalez has attained degrees from Sam Houston State University, Southwest Texas State University, University of Houston, Corpus Christi State University, and Laredo State University. He has experience in law enforcement, social work, education, and school administration. He served as Principal for Martin HS and Lara Academy prior to his retirement. At the present time, he is the Community Outreach Coordinator for Si Texas-Juntos for Better Health with TAMIU. He is married to the former Ruby Smith, has two children, and four grandchildren.
References
Adler, N.E., Cutler, D.M., Fielding, J.E., Galea, S., Glymour, M.M., Koh, H.K., and Satcher, D. (2016). Addressing social determinants of health and health disparities. National Academy of Medicine. Retrieved from https://nam.edu/wp-content/uploads/2016/09/Addressing-Social-Determinants-of-Health-and-Health-Disparities.pdf
Braveman, P. & Gottlieb, L. (2014). The social determinants of health: It's time to consider the causes of the causes. Public Health Reports. 129(1, Suppl2): 19-31. doi:10.1177/00333549141291S206
Center for Disease Control. (2017). National Diabetes Statistics Report, 2017. Retrieved from https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf
Egerter S, Braveman P, Sadegh-Nobari T, Grossman-Kahn R, Dekker M. Education matters for health: Exploring the social determinants of health: issue brief no 6. Retrieved from http://www.commissiononhealth.org/PDF/c270deb3-ba42-4fbd-baeb-2cd65956f00e/Issue%20Brief%206%20Sept%2009%20-%20Education%20and%20Health.pdf
Ehrenfeld, R.M. (1919). The evolution of public health nursing. American Journal of Nursing 20(1). pp 14-18.
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a Brief Depression Severity Measure. Journal of General Internal Medicine, 16(9), 606–613. Retrieved from http://doi.org/10.1046/j.1525-1497.2001.016009606.x
Laredo/Webb County Community Needs and Workforce Assessment. (2013). Healthy Laredo: Evolution and future of health disparity community. Retrieved from https://issuu.com/graphitiks/docs/needs_assessment_report_2optimized_61b426b97885f8
Mandel, A. (2014, August 6). Disparities in access to health care. News Medical Life Sciences. Retrieved from https://www.news-medical.net/health/Disparities-in-Quality-of-Health-Care.aspx
Mobile Health Map. (2016). A literature review of the scope & impact of mobile health clinics. Harvard Medical School. Retrieved from https://static1.squarespace.com/static/509ab226e4b058edb8efe5a9/t/592ed75bc534a537fbb91943/1496242030963/A+Literature+Review+of+the+Scope+and+Impact+of+Mobile+Health+Clinics+2016.pdf
Parkerson, G., Broadhead, W., & Tse, C. (1990). The Duke Health Profile: A 17-Item Measure of Health and Dysfunction. Medical Care, 28(11), 1056-1072. Retrieved from http://www.jstor.org/stable/3765217
Robert Wood Johnson Foundation. (2009). Advancing diabetes self management. Retrieved from http://www.diabetesinitiative.org/programs/DIGateway.html
Texas Department of State Health Services. (2015). The burden of diabetes in Texas. Austin, TX: Office of Surveillance, Evaluation, and Research Health Promotion and Chronic Disease Prevention Section Texas Department of State Health Services.
United States Census Bureau. (2014, December 28). ABCs demographic and housing estimates 2013. Retrieved from U.S. Census Bureau's American Community Survey Office: www.census.gov
University of Wisconsin Population Health Inst. (2015, June 15). County health rankings 2015. Retrieved from: http://www.countyhealthrankings.org/sites/default/files/state/downloads/2015CountyHealthRankingsTexasData-v1_0.xls
Yu, S. Y., Hill, C., Ricks, M. L., Bennet, J., & Oriol, N. E. (2017). The scope and impact of mobile health clinics in the United States: A literature review. International Journal for Equity In Health, 16(1), 178. doi:10.1186/s12939-017-0671-2